Artificial intelligence for pharmacists uses intelligent systems to review prescriptions, detect drug interactions and dosage risks, and support safer medication decisions by helping pharmacists analyze information quickly while retaining full clinical responsibility.
Pharmacy today is becoming more complex than it used to be. Patients often take multiple medicines at the same time; treatments are more specialized, and pharmacists are expected to check prescriptions quickly while still ensuring safety. Reviewing drug combinations, correct doses, and possible risks within a busy workflow is not always easy, especially when large amounts of information need to be considered at once.
This is where AI in pharmacy is beginning to support pharmacists. Artificial intelligence in pharmacy does not replace professional judgment or decision-making. Instead, it helps by scanning information quickly, highlighting possible risks, and bringing attention to details that may need closer review. The pharmacist still makes the final decision, but the process becomes faster and more structured.
For life science graduates entering pharmacy or healthcare roles, understanding how AI in pharmacy supports everyday pharmacy work is becoming increasingly important. As medicines and treatment approaches continue to evolve, pharmacists are expected not only to dispense medicines accurately but also to play a stronger role in medication safety. AI in drug discovery is gradually becoming one of the tools that helps make this possible.
Where AI Fits in Everyday Pharmacy Practice
AI in pharmacy is becoming useful mainly at the point where pharmacists review prescriptions and ensure medication safety. In daily practice, pharmacists often need to check multiple factors at the same time, including drug combinations, dosing accuracy, therapy duration, and patient-related risks. When prescriptions are reviewed under time pressure, important details can sometimes be overlooked even with careful manual checking.
Clinical decision support AI systems support this process by reviewing prescription information within seconds and highlighting situations that may require closer attention. Instead of replacing the pharmacist’s role, AI acts as an additional layer of review that helps organize information and reduce the chances of missing critical risks. This allows pharmacists to focus more on clinical judgment and communication rather than repetitive checking.
In practice, AI in prescription analysis is most visible in three areas of routine pharmacy work. It helps identify potential drug interactions, detect unusual or unsafe dosing, and recognize therapy-related risks such as duplicate medicines or long-term safety concerns. These functions are not separate from normal pharmacy responsibilities; they strengthen the existing review process and make medication safety more consistent, especially in busy environments. Additionally, AI supports AI in medication management to improve overall workflow and patient safety.
AI in Prescription Analysis: Improving Medication Safety in Everyday Practice
Prescription review is one of the most important responsibilities in pharmacy practice. Before medicines reach the patient, pharmacists must check whether the treatment is appropriate, safe, and free from avoidable risks. This includes reviewing drug combinations, confirming correct doses, and identifying therapy choices that may cause harm in certain patients. As prescriptions become more complex, completing this review accurately within a limited time can be challenging.
AI in prescription analysis supports prescription review by quickly scanning prescription details and comparing them with available medical knowledge and safety guidelines. Instead of manually checking every possibility, pharmacists receive alerts when something appears unusual or potentially risky. This allows attention to be directed toward prescriptions that require closer evaluation, improving both speed and accuracy in routine workflows.
One of the most common uses of AI in pharmaceuticals is detecting drug interactions. Some medicines can change how others work in the body, increasing the risk of side effects, or reducing treatment effectiveness. AI systems automatically review medicine combinations and flag interactions that may need monitoring or clarification before dispensing. This helps pharmacists identify risks early and prevent avoidable complications.
AI also helps detect dosage-related problems. A dose that is too high or too low can be dangerous, especially for elderly patients, children, or individuals with kidney or liver conditions. By comparing prescribed doses with standard recommendations and known safety ranges, AI can highlight prescriptions that appear unusual. The pharmacist can then recheck the prescription or consult the prescriber if needed. Using data-driven comparison models like those used in predictive modeling in drug development, the system identifies unusual prescriptions quickly.
Beyond individual medicines, AI can review the overall therapy plan. It may identify duplicate medicines from the same drug class, unnecessary overlaps in treatment, or long-term therapy risks that are not immediately obvious. By looking at the prescription rather than isolated drugs, AI helps pharmacists make safer and more informed decisions.
In this way, AI does not replace professional judgments. It strengthens prescription review by acting as a safety layer that supports pharmacists in managing complexity while maintaining patient safety.
PG Diploma in
Intelligent Healthcare Management (iHealth) Training
Develop practical skills to manage healthcare operations using data-driven decision-making, digital tools, and intelligent systems. Learn how modern hospitals, healthcare organizations, and life-science teams optimize processes, quality, and outcomes through technology and analytics.
Healthcare Operations Management, Healthcare Data Interpretation, Digital Health Systems & Workflows, Quality & Compliance Basics, Process Optimization, Healthcare Analytics Fundamentals, Decision-Making Using Real-World Healthcare Data
AI in Drug Discovery: Why It Matters to Pharmacists
Pharmacists are not directly involved in drug discovery, but changes in how medicines are developed still affect everyday pharmacy practice. AI driven drug discovery helps researchers identify drug targets, screen compounds, and evaluate potential treatments faster than traditional methods. Today, AI based drug discovery and machine learning in drug discovery platforms are transforming how treatments are identified in modern medicine.
AI drug discovery also contributes to drug repurposing, where existing medicines are approved for new indications. For pharmacists, this means treatment options continue to evolve at a faster pace. Medicines may be introduced with more specific indications, complex dosing considerations, or new safety profiles that require careful review during prescription analysis. Understanding the pace of innovation in the AI in pharmaceutical industry helps explain why prescription review is becoming more complex over time.
Understanding this shift helps explain why prescription review is becoming more complex over time. As drug development accelerates, the pharmacist’s role as the final safety checkpoint before medicines reach patients becomes even more important. AI therefore supports pharmacists not only at the prescription level but also indirectly by helping manage the growing complexity created by modern drug development.
How AI Is Changing the Role of Pharmacists
As AI becomes part of pharmacy workflows, the role of pharmacists is gradually shifting from routine checking toward deeper clinical involvement. Tasks that previously required repetitive manual verification, such as scanning for interactions or comparing doses with standard references, can now be supported by intelligent systems. This allows pharmacists to spend more time interpreting risks, counseling patients, and communicating with prescribers when changes are needed.
In many healthcare settings globally, pharmacists are already taking on stronger responsibilities in medication review and treatment optimization. AI supports this transition by helping organize information and bringing potential concerns to attention early. Instead of increasing workload, the goal is to reduce cognitive pressure so pharmacists can focus on decision-making rather than data searching.
In India, pharmacy practice has traditionally emphasized accurate dispensing and operational efficiency. However, with the gradual adoption of digital prescriptions, hospital information systems, and electronic records, opportunities for pharmacists to contribute more actively to medication safety are increasing. AI tools can support this shift by strengthening prescription review and helping pharmacists participate more confidently in clinical discussions.
Rather than reducing the importance of pharmacists, AI increases the need for professional judgment. Alerts and recommendations still require interpretation, and patient-specific decisions cannot be automated. The pharmacist remains responsible for ensuring that treatment is safe, appropriate, and clearly understood by the patient.
Preparing for an AI-Supported Pharmacy Environment
Pharmacy practice is gradually moving toward a model where safety, review, and clinical decision-making play a larger role than routine dispensing alone. As prescriptions become more complex and treatment options evolve faster, pharmacists are expected to manage increasing amounts of information while maintaining accuracy and patient safety. AI is becoming part of this transition by helping organize information, highlight risks, and support more consistent prescription review. The responsibility for decisions, however, continues to remain with the pharmacist.
For life science graduates and pharmacy professionals, this shift means that understanding digital systems and AI-supported workflows is becoming increasingly relevant. Pharmacists who are comfortable working with decision-support tools are better prepared to interpret alerts, communicate risks clearly, and contribute more actively to patient care. Rather than changing the purpose of the profession, AI is strengthening the pharmacist’s role as the final safety checkpoint before medicines reach patients.
To support this transition, CliniLaunch Research Institute offers the Intelligent Healthcare Management (iHealth) training program, designed to help healthcare and life science professionals understand how digital systems, healthcare data, and AI applications fit into modern healthcare operations. The program focuses on practical exposure to healthcare workflows, decision-making using data, and the operational side of intelligent healthcare systems, helping learners build confidence in working alongside evolving technologies.
As healthcare continues to integrate intelligent systems into everyday practice, pharmacists who adapt early will be better positioned to handle complex therapies, support safer treatment decisions, and grow into more clinically involved roles within the healthcare ecosystem.
Frequently Asked Questions (FAQs)
1. What is AI for pharmacists in simple terms?
AI for pharmacists refers to software systems that assist in reviewing prescriptions by identifying potential risks such as drug interactions, incorrect dosing, or duplicate therapies. It acts as a decision-support tool that helps pharmacists work more efficiently while maintaining patient safety.
2. Does AI replace pharmacists in pharmacy practice?
No. AI does not make final decisions or replace professional judgment. It highlights possible risks and organizes information, but pharmacists remain responsible for evaluating prescriptions, interpreting alerts, and ensuring safe medication use.
3. How does AI help in prescription analysis?
AI helps by automatically reviewing medicine combinations, checking dose ranges against safety guidelines, and identifying therapy overlaps or long-term risks. This allows pharmacists to focus on clinical evaluation rather than manual checking.
4. Can AI detect drug interactions accurately?
AI systems can quickly compare prescribed medicines against large medical databases and flag known interaction risks. However, pharmacists must still interpret whether the interaction is clinically significant for a specific patient.
5. Why should life science graduates learn about AI in pharmacy?
Pharmacy and healthcare workflows are becoming increasingly digital. Understanding how AI-supported systems work helps life science graduates adapt to modern healthcare environments and participate more effectively in medication safety and clinical decision-making.
6. Is AI used in pharmacies in India today?
AI adoption varies across settings, but digital prescription systems, hospital information systems, and clinical decision-support tools are gradually becoming more common. AI is increasingly used to strengthen prescription review and reduce medication errors.
7. What skills do pharmacists need in an AI-supported environment?
Pharmacists do not need programming skills. More important skills include understanding digital workflows, interpreting AI-generated alerts, applying clinical judgment, and communicating medication risks clearly to patients and prescribers.
8. How is AI in drug discovery relevant to pharmacists?
Pharmacists are not involved in drug discovery itself, but AI-driven research leads to faster introduction of new medicines and new uses for existing drugs. This increases the importance of careful prescription review and staying updated with evolving therapies.
9. What is the biggest benefit of AI for pharmacists?
The main benefit is reduced cognitive load. AI helps manage large amounts of prescription information quickly, allowing pharmacists to focus more on safety, patient counseling, and clinical decision-making.
10. How can pharmacists prepare for AI-driven healthcare workflows?
Pharmacists can prepare by developing digital literacy, understanding how decision-support systems function in healthcare settings, and gaining exposure to data-driven healthcare operations and modern medication safety practices.
Clinical Project Associate
A Clinical Project Associate (CPA) supports clinical trial operations by managing study documentation,
coordinating project activities, supporting sites and vendors, and ensuring compliance with GCP and
regulatory standards. The role serves as an entry point into clinical research operations and project
management.
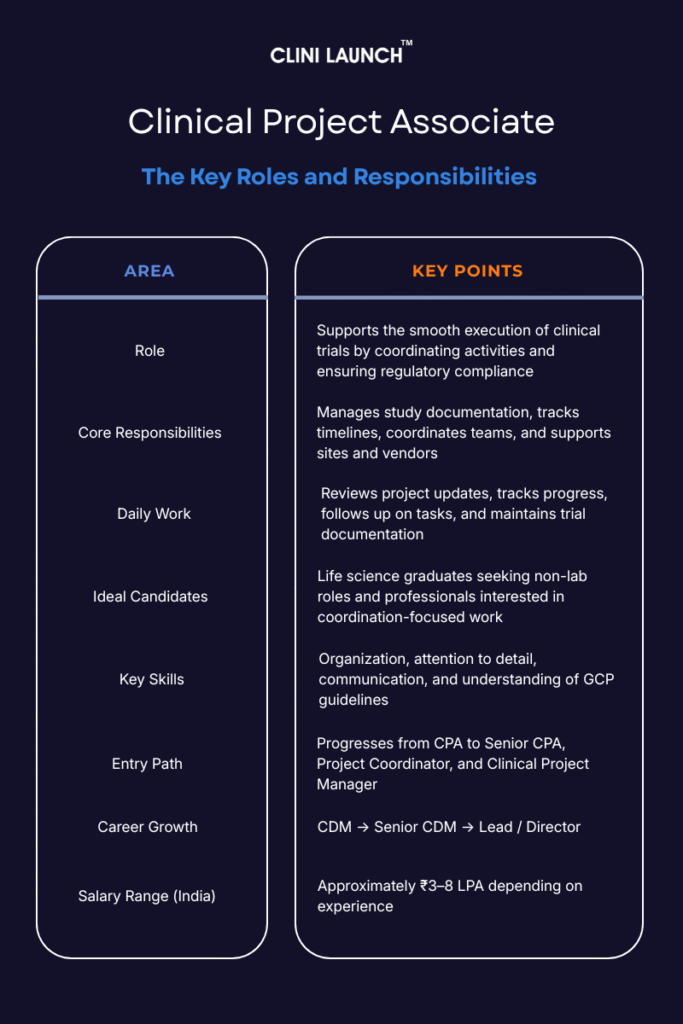
A Clinical Project Associate (CPA) supports the execution of clinical trials by assisting Clinical Project Managers with core operational tasks. The role primarily involves managing study documentation, tracking project timelines, coordinating activities across sites and teams, and supporting regulatory compliance throughout the clinical trial lifecycle.
CPAs work across multiple phases of a clinical trial and support routine operational workflows that help maintain alignment with planned study processes. Their involvement spans different trial stages, ensuring continuity across ongoing activities.
Over the past two decades, clinical research roles have become more complex, with greater emphasis on documentation control, timeline tracking, and regulatory compliance. These evolving demands closely align with the core responsibilities of Clinical Project Associates.
A Clinical Project Associate (CPA) supports clinical trial operations by managing study documentation, coordinating project activities, supporting sites and vendors, and ensuring compliance with GCP and regulatory standards. The role serves as an entry point into clinical research operations and project management.
Who Is a Clinical Project Associate (CPA)?
A Clinical Project Associate is a central operational professional within the clinical trial team who ensures consistency, coordination, and control across trial activities. CPAs act as a link between project managers, clinical sites, vendors, and internal teams, enabling smooth communication and task execution.
The importance of the CPA role lies in its ability to prevent delays, reduce errors, and maintain audit readiness. By keeping documentation accurate, timelines visible, and communication aligned, CPAs help ensure that clinical trials move efficiently from study start-up to close-out, supporting the timely development of new treatments.
CPA vs CRA: Understanding the Difference
While both roles support clinical trials, Clinical Project Associates (CPAs) and Clinical Research Associates (CRAs) have different responsibilities. A CPA focuses on project coordination, documentation, timeline tracking, and operational support, working closely with project managers, sites, and vendors to keep studies organized and compliant.
In contrast, a CRA is primarily responsible for site monitoring activities, including site visits, source data verification, and ensuring protocol adherence at investigational sites. CRAs work directly with trial sites, while CPAs operate more from a central, coordination-based role.
In simple terms, CPAs manage trial operations from behind the scenes, while CRAs oversee trial conduct at the site level.
Core Roles and Responsibilities of a CPA
A CPA is responsible for supporting the coordination and smooth execution of clinical trials, ensuring that operational tasks are completed efficiently, on schedule and in compliance with regulatory standards. CPA roles and responsibilities include supporting documentation, timelines, coordination, and compliance. Below are the core roles and responsibilities of a CPA:
1.Clinical Trial Documentation Oversight
Clinical trials generate large volumes of documents, and even minor documentation errors can delay approvals or trigger audit findings. CPAs are responsible for ensuring that every document is accurate, complete, current, and compliant with regulatory standards.
They help prepare, organize, and maintain essential study documents such as protocols, informed consent forms, investigator brochures, and regulatory submissions. By properly indexing and maintaining study master files, CPAs make sure that documents are easily retrievable during audits, inspections, or sponsor reviews. These clinical project associate duties form the foundation of trial documentation control. This process ensures effective project documentation management throughout the study.
Task
Explanation
Ensure Regulatory Compliance of Documents
CPAs ensure clinical trial documents are accurate, complete, and compliant with GCP and regulatory standards.
Prepare and Organize Study Files
CPAs prepare and organize study documents (e.g., protocols, consent forms) and ensure proper indexing and storage for easy audit access.
Trial Master File (TMF) Maintenance
CPAs organize and index study documents to maintain the TMF and ensure readiness for audits and inspections.
2. Project Coordination and Timeline Management
Clinical trials run on strict timelines, and delays at any stage can impact costs, patient recruitment, and regulatory submissions. CPAs support project managers by tracking milestones, monitoring progress, and flagging risks early.
They coordinate activities across teams, help organize meetings, and ensure that assigned tasks are completed as planned. When delays occur, CPAs assist in identifying the cause and work with the team to adjust timelines or re-prioritize activities.
Task
Explanation
Track Project Progress
CPAs ensure project milestones are achieved on time and assist in adjusting plans if there are delays.
Monitor Project Timelines
CPAs ensure tasks remain on schedule and adjust timelines when necessary to meet project goals.
Coordinate Team Activities
CPAs organize team meetings and ensure activities align with project objectives and deadlines, keeping all team members on track.
Identify and Address Delays
CPAs proactively identify delays and collaborate with the team to resolve issues quickly.
3. Site Operations & External Partner Coordination
Clinical trial sites and vendors play a crucial role in study execution, and CPAs support their readiness and compliance. During site initiation, CPAs help ensure that all required documents, supplies, and systems are in place before patient enrolment begins. Vendor coordination is a core responsibility during trial execution.
They also assist in tracking site performance metrics, monitoring protocol adherence, and identifying compliance issues. When deviations or gaps are observed, CPAs support follow-up actions and documentation. CPAs play a key role during study start up activities at trial sites.
Task
Explanation
Support Site Initiation and Setup
CPAs prepare clinical trial sites with required documents, supplies, and equipment to ensure readiness for patient enrolment.
Monitor Site Performance and Compliance
CPAs monitor site activities to ensure protocol compliance, track performance metrics, and address any non-compliance issues.
CPA may not be the right fit if you prefer working independently with minimal coordination, or if frequent follow-ups, timelines, and documentation feel draining. But if you’re organized, proactive, and enjoy keeping complex clinical work on track, this role can be a strong and rewarding starting point in the industry.
4.Data Collection Support & Study Reporting Assistance
Accurate and complete data is the foundation of every clinical trial outcome. CPAs assist in data collection, data entry, and verification, ensuring that trial data is consistent, traceable, and ready for analysis. These activities contribute to ongoing regulatory compliance support.
They also support the preparation of progress reports, safety reports, and final study reports that are reviewed by sponsors and regulatory authorities. While they may not perform statistical analysis, CPAs ensure that data flows correctly from sites to databases and into reports without gaps or inconsistencies.
Task
Explanation
Assist in Data Collection and Entry
CPAs ensure accurate data collection, entry, and verification while maintaining data completeness and consistency.
Support Report Preparation
CPAs assist in preparing progress, safety, and final study reports for review by sponsors and regulatory authorities.
5.Clinical Trial Team Coordination & Information Flow
Clinical trials involve multiple stakeholders project managers, monitors, investigators, sponsors, vendors, and internal teams. CPAs act as communication facilitators, ensuring that information flows clearly and on time.
They organize meetings, circulate updates, track action items, and prepare status reports that help teams stay informed. By supporting internal communication, CPAs reduce confusion, prevent misalignment, and help teams respond quickly to changes or issues.
Task
Explanation
Cross-functional Team Coordination
CPAs coordinate team communication by organizing meetings and sharing project information with stakeholders, sponsors, and site teams.
Support Internal Project Team
CPAs support internal project teams with updates, status reports, and clear communication to ensure access to necessary project information.
6. Protocol, GCP Training Support & Regulatory Awareness
CPAs play a supportive role in training site personnel and internal teams on study protocols, GCP requirements, and trial processes. This ensures that everyone involved understands their responsibilities and follows standardized procedures. This ensures consistent SOP adherence across study teams.
In addition, CPAs are expected to continuously stay updated on regulatory changes, evolving trial methodologies, and industry best practices. This ongoing learning helps them maintain compliance and contribute effectively to trial execution.
Task
Explanation
Assist with Training Site Personnel
CPAs train site staff and project teams on study protocols, GCP standards, and processes to ensure compliance and data accuracy.
Stay Updated with Industry Regulations
CPAs stay informed about regulatory changes, trial methodologies, and industry standards to maintain ongoing compliance.
PG Diploma in
Clinical Research
Gain in-depth understanding of how clinical trials operate across pharma companies, CROs, and research sites. This program focuses on the practical execution of clinical studies, ethical conduct, documentation, and regulatory compliance across the clinical trial lifecycle.
Day in the Life of a Clinical Project Associate (CPA)
A Clinical Project Associate begins the day by checking project updates and understanding what needs to be completed to keep the clinical trial on track. They review timelines, follow up on pending tasks, and ensure that study activities are progressing as planned.
As the day continues, the CPA focuses on organizing and updating study documents. Trial files are reviewed for accuracy, new documents are filed correctly, and everything is kept ready for audits and inspections. Documentation control remains a constant responsibility throughout the day.
The CPA then supports coordination between teams by sharing updates, tracking action items, and assisting with meeting follow-ups. Communication with clinical sites and external partners helps ensure that study requirements are met and any issues are documented and addressed.
Before the day ends, the CPA updates trackers and reports, ensuring that all activities are recorded and visible to the project team. By maintaining order, coordination, and compliance, the CPA helps the clinical trial move forward smoothly.
Who Can Become a Clinical Project Associate?
A bachelor’s degree in life sciences, health sciences, pharmacy, nursing, or a related field is required for the role. A master’s degree, such as an MSc in Clinical Research or an MPH, is preferred for more advanced or competitive positions. Certifications or training in clinical research, project management, or regulatory compliance (e.g., GCP certification) are also valuable. Additionally, some prior experience in clinical trial operations, clinical research coordination, data management, or a related field is beneficial.
This role requires strong organizational and communication skills, attention to detail, and basic project management abilities essential for clinical project associate jobs. Knowledge of ICH GCP guidelines with trial tools (CTMS, spreadsheets) are essential for compliance. Adaptability and problem-solving skills are also crucial for managing changing trial demands and operational issues. Familiarity with a clinical trial management system is beneficial.
Conclusion
Clinical Project Associates (CPAs) play a vital role in the smooth execution of clinical trials. They manage key tasks such as documentation, project coordination, site management, and data handling, ensuring that trials stay on track and comply with regulatory standards. CPAs are essential to maintaining trial efficiency, reducing delays, and supporting the timely delivery of new treatments. Their contributions are indispensable for the successful progression of clinical research, making them integral to the overall success of clinical trials.
If you’re interested in pursuing a career in clinical research and becoming a vital part of clinical trials, the PG Diploma in Clinical Research by Clinilaunch providing excellent opportunity to gain the knowledge and skills needed to succeed.
FAQ:
1. Do CPAs work on multiple clinical trials at the same time?
Yes. CPAs often support more than one study simultaneously, depending on trial complexity and organization structure. This helps them gain broader exposure to different trial phases and processes.
2. Is prior industry experience mandatory to become a CPA?
No. Many organizations hire freshers or trained candidates for CPA roles. Relevant training, understanding of clinical trial workflows, and documentation practices are often more important than prior experience.
3. Do CPAs interact directly with regulatory authorities?
CPAs usually do not communicate directly with regulatory authorities. However, they support regulatory submissions and documentation that are reviewed by sponsors or regulatory teams.
4. Can CPAs work in remote or hybrid roles?
Yes. Many CPA roles are office-based or remote, especially in CROs and sponsor companies, as the work primarily involves coordination, documentation, and system-based activities.
5. How is a CPA’s performance usually evaluated?
Performance is commonly assessed based on documentation accuracy, timeline adherence, task follow-up, communication quality, and audit readiness support rather than field-based activities.
6. Is the CPA role more administrative or technical?
The CPA role is operational rather than purely administrative. It requires understanding clinical trial processes, regulatory expectations, and coordination of workflows, not just routine office work.
7. Do CPAs need strong technical or programming skills?
No programming skills are required. Basic proficiency in spreadsheets, document management systems, and clinical trial tools is sufficient for most CPA roles.
8. Can a CPA transition into non-project roles later?
Yes. With experience, CPAs can move into regulatory affairs, trial operations, quality assurance support, or training roles within clinical research organizations.
9. Is the CPA role the same across all companies?
Core responsibilities remain similar, but the exact scope can vary between sponsors, CROs, and research sites depending on organizational structure and trial scale.
10. How long does it usually take to grow from CPA to a senior role?
Typically, professionals can progress to senior or coordination roles within 2–4 years, depending on performance, exposure to multiple studies, and organizational opportunities.
The role of a Clinical Data Manager (CDM) is to make sure clinical trial data is accurate, complete, and compliant. Clinical Data Managers set up EDC systems, design CRFs, check data quality, manage queries, and support database lock so the data can be safely analyzed and reviewed by regulators.
Behind every successful clinical trial and every approved drug is one non-negotiable factor: reliable data. If trial data is incomplete, inconsistent, or non-compliant, the study fails, regardless of how promising the drug looks. This is where the role of clinical data manager becomes critical. In clinical data management, CDMs are responsible for ensuring that data collected from study sites is accurate, traceable, and ready for regulatory scrutiny.
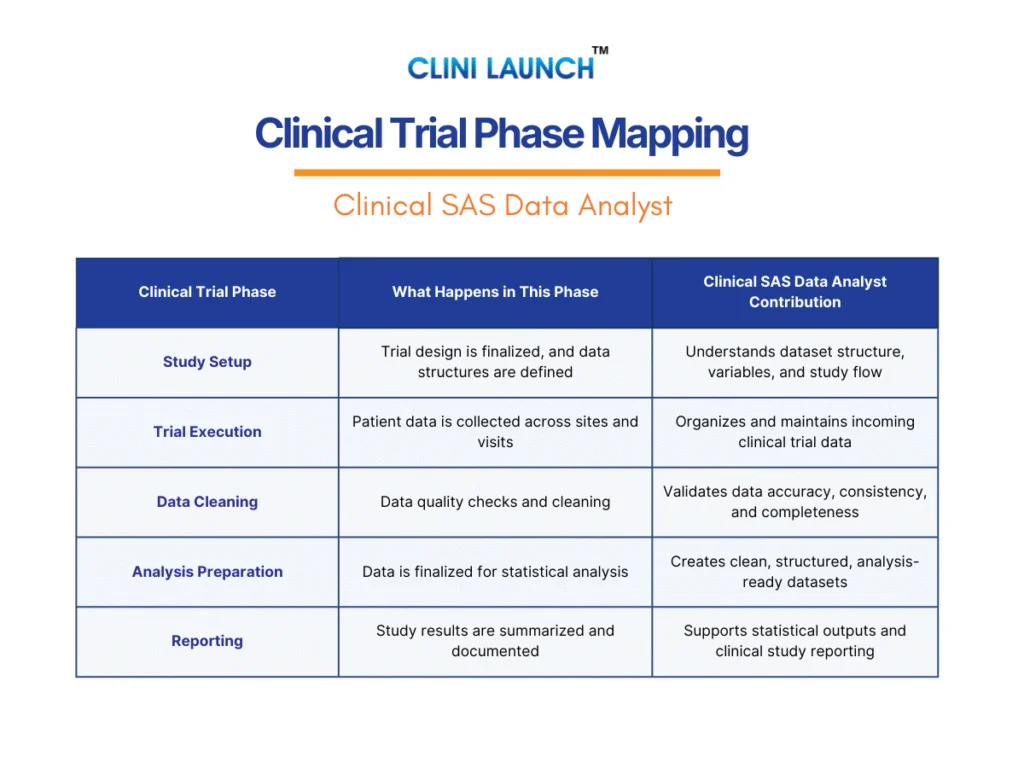
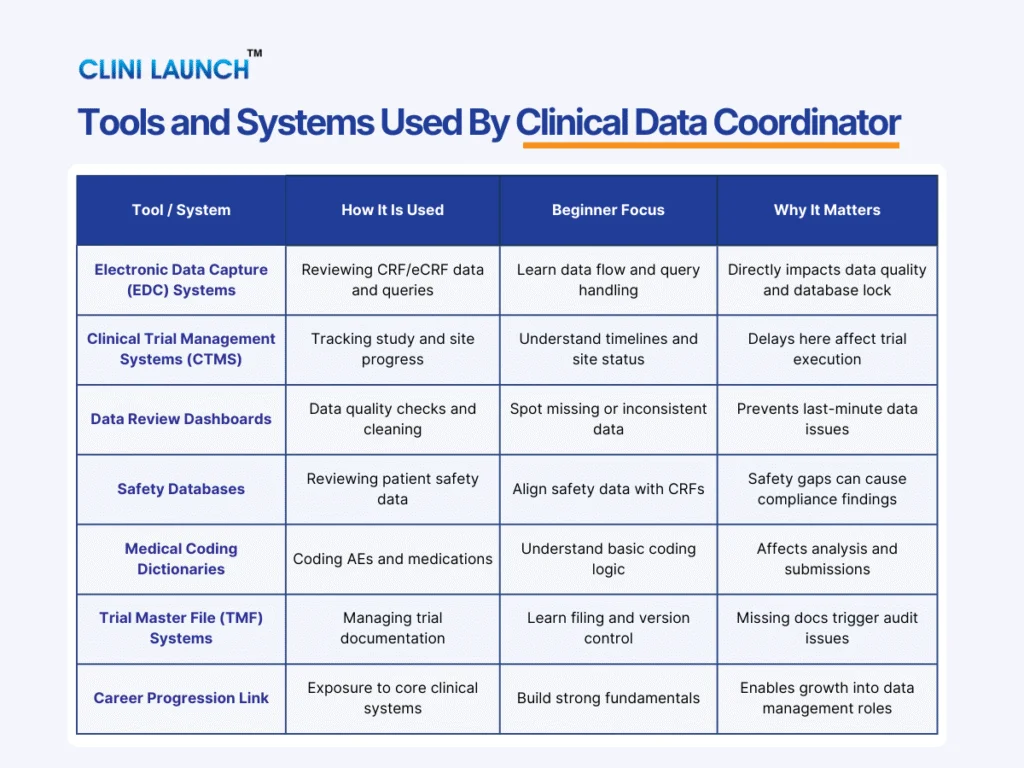
Clinical data management is not about analysis or statistics. It is about control. From designing data collection tools like Case Report Forms (CRFs/eCRFs) and configuring Electronic Data Capture (EDC) systems, to running data validation checks, managing queries, and supporting database lock, the role of clinical data manager in clinical trials spans the entire data management lifecycle. Their work directly impacts data quality assurance, patient safety data, and the credibility of study results.
In clinical data management in clinical research, CDMs act as the operational backbone between clinical teams, CRAs, and biostatistics. They ensure trial data follows the protocol, meets ICH-GCP compliance, and aligns with regulatory requirements in clinical research. In simple terms, the clinical data manager job role exists to turn raw clinical trial data into clean, compliant, submission-ready datasets that regulators can trust.
Who is a Clinical Data Manager?
A Clinical Data Manager (CDM) is a clinical research professional responsible for controlling, reviewing, and preparing clinical trial data so it is accurate, consistent, and compliant with regulatory standards.
In clinical data management in clinical trials, data is collected from multiple sites, investigators, and external sources. Without proper oversight, this data can become incomplete or inconsistent. The Clinical Data Manager prevents this by managing how data is captured in Electronic Data Capture (EDC) systems, applying validation rules, performing data cleaning in clinical trials, and resolving issues through structured query management.
The role of clinical data management is not to interpret results or perform analysis. Instead, CDMs focus on clinical trial data integrity and process control. They execute the Data Management Plan, ensure ICH-GCP compliance, and support audit and inspection readiness. By supporting database lock and maintaining inspection-ready documentation, the clinical data manager responsibilities ensure trial data remains reliable from first patient visit to final submission.
What Does a Clinical Data Manager Do in a Trial?
A Clinical Data Manager (CDM) is responsible for overseeing how data is collected, reviewed, cleaned, and prepared throughout a clinical trial in line with regulatory standards. From the first patient visit to final database lock, the role of clinical data manager is to ensure that trial data is accurate, complete, consistent, and compliant.
During a trial, the CDM designs and manages data collection tools such as Case Report Forms (CRFs) and Electronic Data Capture (EDC) systems, ensuring they align with the study protocol. As data is entered by clinical sites, the CDM continuously monitors it for missing values, inconsistencies, and protocol deviations, raising and resolving queries with sites as part of structured query management to maintain data quality.
The CDM also coordinates closely with clinical operations, biostatistics, and regulatory teams, highlighting the collaborative nature of the clinical data manager job role. By validating datasets, enforcing data standards, and supporting audits and inspections, the role of clinical data manager is central to transforming raw trial data into reliable evidence for regulatory submissions and drug approvals.
PG Diploma in
Clinical Research
Gain in-depth understanding of how clinical trials operate across pharma companies, CROs, and research sites. This program focuses on the practical execution of clinical studies, ethical conduct, documentation, and regulatory compliance across the clinical trial lifecycle.
Core Roles and Responsibilities of Clinical Data Manager (CDM)
EDC Configuration and Validation
Before a clinical trial starts, a Clinical Data Manager’s first responsibility is to set up the system where all study data will be entered and stored. This system is called an Electronic Data Capture (EDC) system. The CDM does not build the software, but decides how the study will use it. This includes designing Case Report Forms (CRFs or eCRFs), which are the forms used by trial sites to enter patient data. Each form is created based on the study protocol so that the right data is collected at the right visit, in the right format.
The Clinical Data Manager also controls how data can be entered into the system. They define which fields are mandatory, what type of values are allowed, and what ranges are acceptable. For example, a heart rate field should only accept realistic numbers, and important fields should not be left blank. The CDM sets up validation rules, also called edit checks, that automatically flag or stop incorrect data at the time of entry. This helps prevent mistakes before they become bigger problems later in the trial.
Before the study goes live, the Clinical Data Manager carefully tests the EDC system to make sure everything works as expected. They check that forms appear correctly, validation rules trigger properly, and data changes are tracked through audit trails. This early setup and testing is critical because well-designed systems reduce errors, limit unnecessary queries, and make data cleaning and database lock much easier later. In simple terms, good EDC configuration ensures that clinical trial data starts clean and stays controlled from day one.
Area
What the CDM Does
Why It Matters
EDC Setup
Configures how the study uses the Electronic Data Capture system
Ensures all sites enter data in a consistent structure
CRF Design
Designs CRFs/eCRFs based on the study protocol
Makes sure the right data is collected at the right visit
Field Definitions
Defines mandatory fields, formats, ranges, and dropdowns
Prevents incorrect or unusable data entry
Edit Checks
Sets up validation rules to flag or block errors
Catches mistakes at entry instead of cleaning later
System Testing
Tests forms, rules, and audit trails before go-live
Avoids data entry issues during live trial
Data Control
Ensures traceability through audit trails
Protects data integrity and inspection readiness
2. Data Quality and Query Management
Once a clinical trial starts and sites begin entering data into the EDC system, the Clinical Data Manager’s primary responsibility shifts to monitoring data quality. This means regularly reviewing the data entered by sites to ensure it is complete, consistent, and logically correct. The CDM checks whether required fields are filled, values make medical sense, and data aligns with the study protocol and visit schedule.
When issues are found, the Clinical Data Manager raises data queries in the EDC system. A query is a formal question sent to the study site asking them to correct, confirm, or explain a data entry. For example, if a patient’s visit date is entered before the informed consent date, or if a lab value is missing, the CDM generates a query so the site can review the source documents and respond. This process is known as query management and continues throughout the trial.
As sites respond to queries, the CDM reviews the updates and confirms whether the issue has been properly resolved. This ongoing cycle of review, query generation, and resolution is called data cleaning in clinical trials. Effective data quality management ensures that errors are fixed early, data trends remain reliable, and the final dataset is ready for database lock and analysis. In simple terms, this role ensures that clinical trial data stays trustworthy as it is being collected, not months later.
Area
What the CDM Does
Why It Matters
Data Review
Regularly reviews data entered by trial sites
Identifies errors early while they are easier to fix
Missing Data Checks
Detects incomplete or skipped fields
Prevents gaps in critical trial data
Consistency Checks
Looks for illogical or conflicting values
Ensures medical and protocol accuracy
Query Generation
Raises queries in the EDC system
Prompts sites to correct or confirm data
Query Tracking
Follows up on open queries and timelines
Prevents delays in data cleaning
Data Cleaning
Confirms issues are resolved correctly
Delivers clean, reliable datasets for analysis
3. Compliance Execution
In clinical trials, data must be collected and handled according to strict rules. A Clinical Data Manager is responsible for executing these rules in daily data work, not creating them. This means ensuring that all data entered, reviewed, and updated in the EDC system follows the study protocol, Good Clinical Practice (GCP), and internal Standard Operating Procedures (SOPs). The CDM’s job is to make sure trial data is handled the right way, every day, without shortcuts.
Compliance execution mainly shows up in how data is controlled and tracked. Clinical Data Managers ensure that every data change is recorded with a clear audit trail showing who made the change, when it was made, and why it was made. They also ensure that access to the EDC system is role-based, patient data is protected, and safety-related data is handled carefully. This is critical because regulators expect full traceability and transparency in clinical trial data.
During audits or inspections, regulators do not just look at the final results. They examine how the data was managed throughout the trial. If data changes cannot be explained or traced, even clean data can be questioned. By consistently following protocol requirements, maintaining audit trails, and supporting inspection readiness, the Clinical Data Manager ensures that trial data remains credible and defensible from start to finish.
Area
What the CDM Does
Why It Matters
Protocol Adherence
Ensures data follows protocol-defined rules
Prevents protocol deviations in trial data
GCP Execution
Applies GCP principles in daily data handling
Protects patient safety and data credibility
SOP Compliance
Follows company data management procedures
Ensures standardized and consistent processes
Audit Trails
Ensures all data changes are tracked and justified
Provides traceability during audits
Data Access Control
Maintains role-based system access
Protects patient confidentiality
Inspection Support
Supports audits and inspections with evidence
Helps trials withstand regulatory review
4. Database Lock Support
As a clinical trial nears completion, all collected data must be finalized so it can be used for statistical analysis. This step is called database lock. A Clinical Data Manager plays a key role in supporting this process by making sure the data is truly ready to be locked. Database lock means no more changes are allowed unless formally justified, so this step requires extreme care.
Before database lock, the Clinical Data Manager performs final data reviews. They check that all critical data has been reviewed, important queries are resolved, missing values are addressed, and discrepancies are explained. They also ensure that data from different sources, such as labs or safety systems, is reconciled and consistent. If even small issues remain unresolved, the database cannot be locked.
The CDM then coordinates with biostatistics and clinical teams to confirm that lock criteria are met. Once the database is locked, the cleaned dataset is handed over for analysis. A smooth database lock reflects strong data management throughout the trial, while delays usually indicate unresolved data quality issues. In simple terms, database lock support is about delivering a final dataset that everyone can trust.
Area
What the CDM Does
Why It Matters
Final Data Review
Reviews all critical trial data
Ensures data is complete and accurate
Query Resolution
Confirms queries are closed or justified
Prevents unresolved issues at lock
Data Reconciliation
Checks consistency across data sources
Avoids mismatched or conflicting data
Lock Readiness Checks
Confirms all lock criteria are met
Ensures the database can be frozen safely
Coordination with Stats
Hands off clean data to biostatistics
Enables accurate statistical analysis
Lock Support
Supports the formal database lock process
Protects trial timelines and submissions
5. Core Documentation
In clinical trials, data is only considered reliable if there is clear documentation showing how it was handled. A Clinical Data Manager is responsible for maintaining the core documents that explain how trial data was collected, reviewed, cleaned, and finalized. This documentation proves that data management activities were performed correctly and consistently throughout the study.
One of the key documents a CDM works with is the Data Management Plan (DMP). The DMP describes how data will be handled during the trial, including data review processes, query management, validation rules, and database lock procedures. The CDM follows and updates this plan as the study progresses. In addition, the CDM maintains system specifications, data handling records, and audit trails that capture all important data-related decisions and changes.
During audits or regulatory inspections, reviewers do not rely on verbal explanations. They expect documented evidence. If data handling steps are not documented, they are treated as if they never happened. By maintaining accurate documentation and supporting inspection readiness, the Clinical Data Manager ensures that trial data can be trusted not only for analysis, but also by regulators reviewing the study.
Area
What the CDM Does
Why It Matters
Data Management Plan
Executes and maintains the DMP
Defines and supports proper data handling
Specifications
Maintains data and system specifications
Ensures consistency and clarity in data setup
Audit Trails
Preserves records of all data changes
Provides traceability and accountability
Documentation Updates
Keeps records current throughout the trial
Reflects real-time data management activities
Audit Support
Provides documents during audits and inspections
Demonstrates compliance and readiness
Data History
Maintains evidence of data handling decisions
Protects data credibility
Conclusion
Clinical Data Management is not a background function. It is the discipline that ensures trial data is accurate, traceable, compliant, and usable. From EDC setup to data quality checks, compliance execution, database lock, and documentation, the role of clinical data manager is operational, detail-driven, and critical to trial success.
For anyone exploring a clinical data manager career, the key takeaway is clear: this role is about systems, processes, and data integrity, not titles. The clinical data manager job description is built on accountability and consistency across the trial lifecycle.
This is where training matters. Clinilaunch Research Institute offers a PG Diploma in Clinical Research focused on real-world clinical trial execution, regulatory expectations, and documentation workflows that support clinical data management in clinical research. For those serious about entering the field with strong fundamentals, it provides a practical starting point.
Frequently Asked Questions – FAQs
1. What does a Clinical Data Manager actually do in a clinical trial?
A Clinical Data Manager controls how trial data is collected, checked, cleaned, and finalized. They configure the EDC system, review data entered by sites, manage queries, ensure compliance, and support database lock so the data can be used for analysis and regulatory submission.
2. Is Clinical Data Management the same as data analysis?
No. Clinical Data Management focuses on data quality and control, not analysis. CDMs prepare clean, compliant datasets. Biostatisticians and analysts use those datasets to perform statistical analysis. If data management fails, analysis cannot even begin.
3. Do Clinical Data Managers work daily with clinical sites?
Yes. CDMs regularly interact with clinical sites through the EDC system by raising and resolving data queries. While they may not speak to sites directly every day, site responses and corrections drive much of a CDM’s daily work.
4. What tools should a beginner CDM learn first?
Beginners should focus on:
Electronic Data Capture (EDC) systems
CRF/eCRF design concepts
Query management workflows
Basics of the Data Management Plan (DMP)
Tool names matter less than understanding how data flows through a trial.
5. Why is database lock so important in CDM?
Database lock freezes the trial data for final analysis. Once locked, changes are heavily restricted. A delayed or poor-quality lock can delay submissions and regulatory timelines. This is why CDMs spend significant effort preparing data before lock.
6. Is Clinical Data Management more operational or managerial?
At its core, CDM is operational. Most CDMs spend their time reviewing data, managing queries, and ensuring compliance. Managerial responsibilities come later with seniority and are not part of the core CDM function.
7. Is CDM a good role for someone who prefers structure over creativity?
Yes. CDM is ideal for people who like structured work, defined rules, and process-driven responsibilities. Success in CDM depends more on accuracy, consistency, and discipline than creative thinking.
8. How difficult is it to move from a junior CDM role to senior roles?
Progression is straightforward if fundamentals are strong. Junior CDMs focus on execution. Senior CDMs take ownership of studies, timelines, and risk. Growth depends on hands-on trial exposure, not just certifications.
9. Does a Clinical Data Manager need to know medical coding or statistics?
Basic awareness helps, but deep expertise is not mandatory at entry level. Coding and statistics are usually handled by specialized teams. CDMs mainly ensure that coded and analyzed data is clean, consistent, and traceable.
10. What makes a Clinical Data Manager “good” at their job?
A good CDM:
Prevents errors through good system setup
Closes queries efficiently
Maintains clean audit trails
Supports smooth database lock
Keeps data inspection-ready at all times
Medical coder roles and responsibilities vary by care setting. Inpatient coding covers full hospital stays, outpatient coding focuses on clinic visits and same-day services, emergency department coding handles urgent care encounters, and ancillary coding supports diagnostic and technical services. Each role differs in documentation depth, decision pressure, and compliance risk.
Medical coding is often misunderstood as a single, routine job where professionals simply convert diagnoses and procedures into codes. In reality, medical coder roles and responsibilities vary significantly depending on where patient care takes place and the type of services delivered. Coding a full hospital admission is fundamentally different from coding a clinic visit, an emergency case, or a diagnostic service, and each carries its own level of complexity, accountability, and regulatory scrutiny.
In real healthcare environments, medical coders play a critical role in ensuring accurate documentation, compliant billing, and smooth functioning of the healthcare revenue cycle. Their work directly affects reimbursement, audit outcomes, and the quality of healthcare data used for reporting and decision-making. Understanding how medical coding responsibilities change across inpatient, outpatient, emergency department, and ancillary settings is essential for anyone exploring medical coding as a career or trying to build realistic job readiness.
This article breaks down who a medical coder is, the different types of medical coding roles that exist, the specific responsibilities attached to each role, and how these responsibilities translate into real day-to-day work inside healthcare organizations.
Who Is a Medical Coder?
A medical coder is a healthcare professional who reviews clinical documentation and converts it into standardized medical codes used for billing, compliance, and reimbursement. Their work directly affects claim accuracy, audit outcomes, and the healthcare revenue cycle.
The duties of a medical coder include interpreting physician notes, discharge summaries, procedure reports, and diagnostic findings, then applying the correct codes based on official guidelines. This role requires accuracy and judgment, not data entry, because coding errors can lead to denials, compliance issues, and revenue loss.
Medical coding is not a single role. Medical coder roles and responsibilities vary depending on where patient care takes place. Based on the care setting, medical coders typically work in:
Inpatient (IP) medical coding – Hospital admissions
Outpatient (OP) medical coding – Clinic visits and same-day services
Emergency department (ED) coding – Urgent and unplanned care
Ancillary medical coding – Diagnostic and technical services
Each role differs in complexity, documentation depth, and work pace. Understanding these differences is essential before learning what responsibilities each role actually carries.
Choosing the Right Medical Coding Role
Aspect
Inpatient (IP)
Outpatient (OP)
Emergency Department (ED)
Ancillary Services
Work pace
Slower and methodical
Steady and consistent
Fast and time-sensitive
Steady and task-focused
Complexity level
High
Moderate
Moderate to high
Moderate
Documentation depth
Very detailed (entire hospital stay)
Moderate (single visit or service)
Brief and evolving
Structured and report-based
Decision intensity
High (multiple diagnoses and procedures)
Moderate (rule-driven decisions)
High (quick judgment required)
Moderate (precision-based decisions)
Entry vs advanced suitability
Better suited after experience
Common entry point for beginners
Entry to intermediate (with guidance)
Entry to intermediate (with structured training)
Who this role fits best
Detail-oriented, analytical learners
Learners who prefer structure
Those comfortable with pressure
Coders who like precision and technical work
Advanced Diploma in
Medical Coding
Build practical skills in medical coding and clinical documentation used across hospitals, healthcare providers, and global healthcare services. Learn how diagnoses, procedures, and services are translated into standardized medical codes while ensuring accuracy, compliance, and reimbursement integrity.
Medical coder roles and responsibilities are defined by where care is delivered, not by job titles. Each role carries different decision pressure, documentation depth, and impact on the healthcare revenue cycle. Treating them as the same role is how beginners get blindsided later.
1.Inpatient Medical Coding (IP)
Inpatient medical coding applies when a patient is formally admitted to the hospital, usually for 24 hours or more. Unlike other roles, inpatient coding covers the entire hospital stay, from admission through discharge.
The coder is responsible for translating a complex clinical journey into codes that accurately reflect:
Why the patient was admitted
What conditions were treated
What procedures were performed
How severe the case was
This role relies heavily on ICD 10 CM coding for diagnoses and ICD-10-PCS for inpatient procedures.
Core Responsibilities
Review the full medical record from admission to discharge
Identify and assign the principal diagnosis
Code all relevant secondary diagnoses, including complications and comorbidities
Apply proper sequencing rules to reflect severity of illness
Code inpatient procedures accurately
Support correct DRG assignment and compliance
Real-world Example:
A Clinical Data Coordinator supports clinical trials by reviewing and coordinating study data to ensure it is accurate, consistent, and inspection-ready. This role covers data review, query coordination, safety data alignment, documentation support, and database lock readiness across the trial lifecycle.
What qualifies as the principal diagnosis
Which secondary diagnoses are reportable
Whether conditions were present on admission or developed later
One wrong decision here doesn’t cause a minor denial. It can shift the DRG entirely and trigger audits.
2.Outpatient Medical Coding (OP)
Outpatient medical coding covers patient encounters where there is no overnight admission. These are high-volume, encounter-based services such as clinic visits, OPDs, and same-day procedures.
Here, speed matters, but accuracy matters more because outpatient claims are aggressively reviewed by payers.
This role uses ICD 10 CM coding, CPT coding, and HCPCS coding extensively.
Core Responsibilities
Code individual visits rather than full hospital stays
Assign diagnosis codes that justify medical necessity
Code procedures and services accurately
Apply modifiers correctly
Ensure diagnosis-to-procedure linkage
Follow payer-specific outpatient coding rules
Real-world Example:
A patient visits a clinic for diabetes follow-up and receives lab tests and medication management.
The outpatient coder must ensure:
The visit level matches documentation
Diagnosis codes support the services billed
Procedures are correctly linked
A missing linkage or incorrect modifier doesn’t look dramatic, but it leads to silent denials and rework.
3.Emergency Department Coding (ED)
Emergency department coding deals with urgent and unplanned care. Documentation is often brief, incomplete, and created while treatment is still happening.
Despite short encounters, ED coding carries high audit risk because visit-level coding is heavily scrutinized.
This role relies on ICD 10 CM coding, CPT coding, and HCPCS coding.
Core Responsibilities
Review triage notes, physician documentation, and treatment records
Assign appropriate visit-level codes
Code emergency procedures accurately
Reflect the severity of the patient’s condition
Work within tight turnaround times
Maintain compliance despite limited documentation
Real-world Example
A patient arrives with chest pain, undergoes rapid evaluation, tests rule out a heart attack, and is discharged.
The ED coder must decide:
What level of evaluation and management applies
Whether documentation supports the billed severity
Which diagnoses are reportable
Overcoding attracts audits. Undercoding loses revenue. There’s no comfort zone.
4 . Ancillary Medical Coding
Ancillary medical coding focuses on diagnostic and technical services, not direct patient visits. This includes labs, radiology, pathology, anesthesia, and similar departments.
This role is precision-driven and largely technical, relying heavily on CPT coding and HCPCS coding.
Core Responsibilities
Review test orders and diagnostic reports
Code technical services accurately
Apply modifiers where required
Ensure services match physician orders
Capture all billable services correctly
Real-world Example:
A patient undergoes multiple lab tests and imaging services on the same day.
The ancillary coder must ensure:
Every test performed is captured
Modifiers reflect how services were delivered
Nothing billable is missed
Errors here don’t cause denials immediately. They cause revenue leakage, which is worse because it often goes unnoticed.
Why This Role Separation Matters
Across all four roles, medical coding job responsibilities directly affect:
Claim outcomes
Audit exposure
Compliance standing
Healthcare revenue cycle performance
This is why medical coding accuracy and medical coding compliance are foundational expectations, not optional skills. Each role tests these skills differently.
AI-augmented Medical Coding and
Revenue Intelligence Certification
Master the intersection of traditional medical coding and cutting-edge AI integration. This isn’t just about memorizing books; it’s about leveraging AI tools to automate workflows, enhance precision, and speed up the coding process in real-world clinical environments. Learn to manage complex data sets while maintaining the high compliance standards required by modern global healthcare systems.
AI-Driven Coding Tools, Automated Medical Indexing, ICD-10-CM/PCS & CPT, Natural Language Processing (NLP) in Healthcare, Data Privacy & Ethics, AI-Assisted Auditing, Electronic Health Record (EHR) Optimization
A medical coder’s day does not follow a single routine. What changes the day completely is which type of coding role the coder works in. While the core responsibility remains accuracy and compliance, the pace, decision pressure, and documentation depth vary sharply across inpatient, outpatient, emergency department, and ancillary medical coding.
This section shows how the roles and responsibilities discussed above translate into actual day-to-day work.
1.Starting the Day: Work Queues Look Different by Role
A medical coder does not “open random charts.” They open role-specific work queues.
Inpatient coders start their day with discharge charts from recent hospital stays. These are fewer in number but heavy in documentation.
Outpatient coders see long queues of clinic visits, OPD encounters, and same-day procedures.
Emergency department coders receive time-sensitive emergency encounters that must be coded quickly.
Ancillary coders work through structured queues of lab tests, imaging studies, pathology cases, or anesthesia records.
Right from the first hour, the difference in medical coding job responsibilities is visible.
2.Reviewing Clinical Documentation: Depth vs Speed
The biggest chunk of a coder’s day is documentation review, but how deep that review goes depends on the role.
In inpatient medical coding, coders read admission notes, progress notes, operative reports, and discharge summaries to understand how the patient’s condition evolved.
In outpatient medical coding, coders review encounter notes and procedure documentation focused on that single visit.
In emergency department coding, coders work with brief, evolving documentation created during urgent care.
In ancillary medical coding, coders review test orders, technical reports, and diagnostic results rather than physician narratives.
This is where clinical understanding matters. The responsibility is not to read everything, but to read what affects coding decisions.
3.Identifying Gaps and Risks in Documentation
Real-world documentation is rarely perfect. A key part of daily work is spotting issues before codes are assigned.
Inpatient coders look for missing specificity, unclear diagnoses, or sequencing issues.
Outpatient and ED coders check whether documentation supports the level of service billed.
Ancillary coders verify that services performed match physician orders and reports.
This step protects medical coding compliance. Guessing is not allowed. If documentation does not support the service, the coder flags it.
4.Assigning Codes: Where Accuracy Is Tested
Once documentation is reviewed, the coder applies the appropriate codes.
ICD 10 CM coding is used across all roles for diagnoses.
ICD-10-PCS is applied by inpatient coders for hospital procedures.
CPT coding and HCPCS coding dominate outpatient, emergency, and ancillary work.
This is where medical coding accuracy becomes non-negotiable. Every incorrect code can lead to denials, audits, or revenue loss. Coders must balance correctness with productivity expectations specific to their role.
5.Balancing Accuracy, Compliance, and Productivity
Every coder works under pressure, but the pressure feels different in each role.
Inpatient coders handle fewer charts but face high financial and audit impact.
Outpatient coders manage high volumes with strict payer scrutiny.
Emergency department coders work against turnaround time with limited documentation.
Ancillary coders focus on precision to avoid missed charges and revenue leakage.
Across all roles, the coder’s decisions directly affect the healthcare revenue cycle. This is why medical coding is not data entry; it is a judgment-driven role.
Conclusion
Medical coding is not a single, uniform job. Across inpatient, outpatient, emergency department, and ancillary settings, medical coder roles and responsibilities differ in documentation depth, decision pressure, work pace, and compliance risk. What remains constant across all roles is the requirement for strong clinical understanding, high medical coding accuracy, and strict medical coding compliance. Coding decisions directly influence claim outcomes, audits, and the healthcare revenue cycle.
As healthcare systems evolve, medical coders are expected to move beyond basic code assignment and develop a deeper understanding of workflows, documentation risks, and revenue impact. This shift is further accelerated by the use of automation and AI-driven tools across healthcare revenue cycle operations.
To support learners at different stages, CliniLaunch Research Institute offers two structured learning paths. The Advanced Diploma in Medical Coding focuses on building strong fundamentals in coding guidelines, clinical documentation analysis, and role-based coding practices across inpatient, outpatient, emergency, and ancillary settings. For learners looking to work at the intersection of coding, data, and automation, the AI-augmented Medical Coding and Revenue Intelligence Course goes a step further by introducing AI-assisted workflows, compliance intelligence, and revenue-focused decision-making.
Understanding how medical coding roles differ helps learners choose the right path, set realistic expectations, and build skills that remain relevant in modern healthcare environments.
FAQs
1. Is medical coding just a data entry job?
No. Medical coding requires interpreting clinical documentation, applying guidelines, and using judgment to ensure accuracy, compliance, and correct billing.
2. What is the difference between IP, OP, ED, and Ancillary medical coding?
The difference depends on where care is delivered. Inpatient covers hospital stays, outpatient handles clinic visits, ED focuses on urgent care, and ancillary coding supports diagnostic services.
3. Which medical coding role is best for beginners?
Outpatient coding is the most common starting point for beginners due to structured documentation and encounter-based workflows.
4. Do all medical coders use the same coding systems?
No. All coders use ICD-10-CM, but inpatient coders also use ICD-10-PCS, while outpatient, ED, and ancillary coders mainly use CPT and HCPCS.
5. Can medical coders move into advanced roles later?
Yes. With experience, coders can move into inpatient coding, QA, HCC, or CDI roles.
6. Why is it important to understand medical coding roles early?
Early role awareness reduces confusion during learning, helps choose the right path, and builds realistic career expectations.
A Clinical Research Coordinator (CRC) supports the execution of clinical trials at the study site. They help coordinate patient visits, manage study documents, support informed consent, assist with data collection, and ensure the study follows the approved protocol and regulatory guidelines.
Imagine a hub where scientific protocols, patient care, documentation, sponsor expectations, and compliance all intersect—that’s where a Clinical Research Coordinator (CRC) comes in. CRCs are the operational heart of clinical studies, ensuring that trials are conducted ethically, efficiently, and in strict accordance with regulations and protocols. Clinical trials are the backbone of modern medicine, and behind every successful trial is a skilled professional managing clinical research coordinator roles and responsibilities to keep studies on track.
Research on clinical trial workforce trends shows that the number of registered clinical trials has increased by over 30%, leading to a growing demand for skilled coordinators. This rise highlights the critical role CRCs play in managing trial complexity and supporting timely, high-quality research outcomes.
In this blog, you’ll discover Clinical Research Coordinator Roles and Responsibilities, what they do every day, and how they manage critical aspects like patient visits and study coordination. Whether you’re a student considering a career in clinical research, a team lead wanting to understand your CRC better, or a manager seeking to optimize your study operations, this guide offers practical clarity on clinical research coordinator roles and responsibilities.
Who is clinical Research coordinator?
A Clinical Research Coordinator (CRC) supports the daily conduct of a clinical trial at the study site. They coordinate study activities, manage documentation, and ensure procedures are followed according to the approved protocol. While the principal investigator oversees medical decisions, the CRC handles site-level coordination, so the trial runs smoothly and in compliance.
CRCs work closely with investigators, study staff, sponsors, and the ethics committee to keep communication clear and timely. They help track study timelines, support patient screening and recruitment, and maintain records, so data remains accurate and audit-ready an essential part of CRC responsibilities in clinical trials.
By managing documentation flow, regulatory requirements, patient coordination, and day-to-day trial activities, the clinical research coordinator roles and responsibilities are central to consistent trial conduct and data accuracy. In many research settings, especially within CRC role in hospitals, CRCs support safety reporting compliance and essential documents maintenance, strengthening overall site operations. Evidence from clinical research settings shows that over 80% of sites report improved trial quality and execution when supported by a dedicated CRC, highlighting the importance of effective job role execution and strict ICH-GCP compliance at the site level. This highlights the importance of the clinical research coordinator job role in maintaining operational control and regulatory alignment at the study site.
Roles and Responsibilities of a Clinical Research Coordinator
This section explains the clinical research coordinator roles and responsibilities across study start-up, conduct, and close-out phases, reflecting real-world expectations outlined in a standard clinical research coordinator for job description.
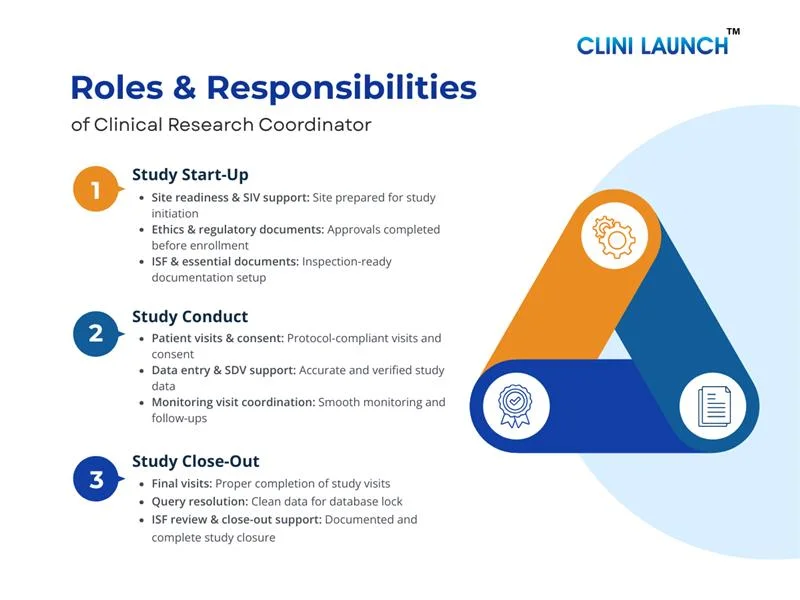
Phase 1: Study Start-Up Phase
The study start-up phase prepares the site before enrollment begins. During this stage, the CRC organizes site readiness and ensures alignment with protocol and compliance requirements.
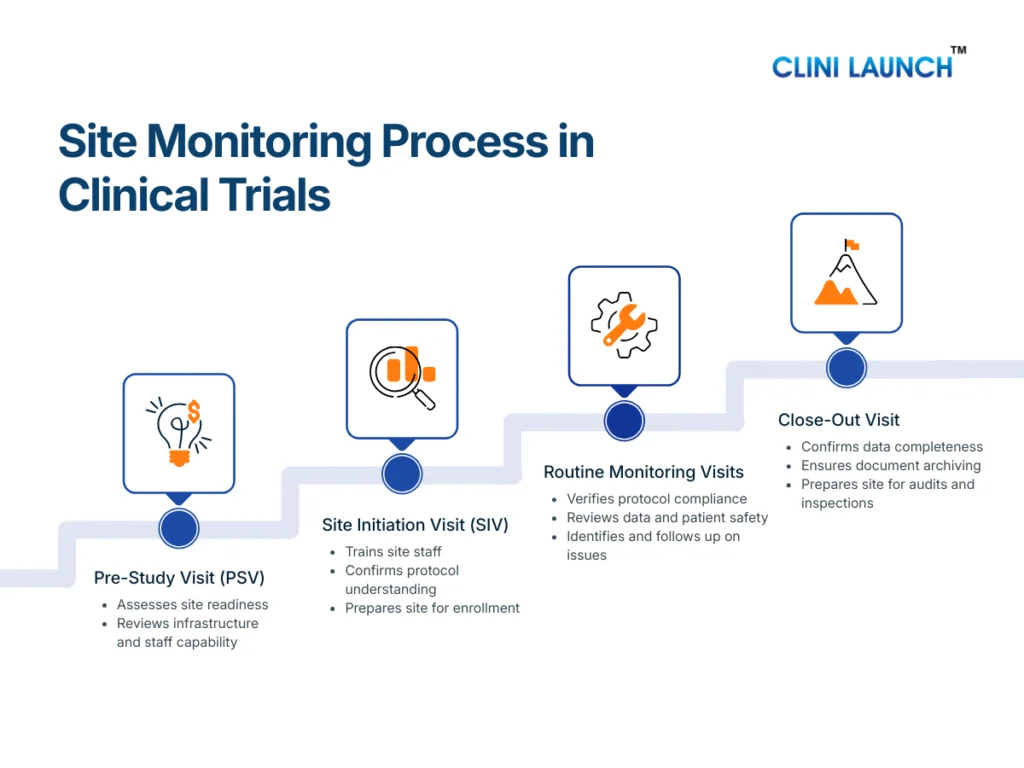
Site Readiness and Study Initiation Support
The CRC supports site readiness by coordinating internal activities, organizing study materials, and assisting with preparation for the Site Initiation Visit (SIV). This ensures the site understands study workflows and is operationally prepared before the trial begins.
Regulatory and Ethics Documentation Support
During start-up, the CRC assists with regulatory and ethics documentation by compiling required records, tracking submission status, and maintaining approval-related correspondence. This helps ensure that all necessary approvals are in place before participant enrollment.
Essential Study Documentation Setup
CRCs organize the trial master file, ISF, delegation logs, training records, and approvals—ensuring inspection of readiness from day one. This ensures documentation is complete, current, and inspection-ready from the start of the study.
CRC Responsibilities During the Study Start-Up Phase
CRC Activity
Purpose
What It Ensures
Site readiness and study initiation support
Prepare the site before trial initiation
Operational readiness and clear workflows
Regulatory and ethics documentation support
Complete required submissions and approvals
Compliance before participant enrollment
Essential study documentation setup
Organize ISF and key study records
Inspection-ready documentation
Case Study: Impact of Protocol Deviations on Clinical Trial Quality
What Happened
Impact
Why CRC Matters
Clinical research literature shows that protocol deviations—departures from the approved study procedures—
frequently occur during the active conduct phase of clinical trials and can compromise both participant
safety and the reliability of trial data. These deviations may include missed assessments, improper
documentation, or procedures conducted outside the defined protocol.
When protocol deviations are not properly identified, recorded, and managed, they can undermine the
scientific validity of a trial, affect data integrity, and potentially jeopardize patient welfare. This
can lead to increased monitoring findings, longer trial completion times, and difficulties during
regulatory review if deviations are widespread or poorly documented.
During the study conduct phase, Clinical Research Coordinators (CRCs) help minimize protocol deviations by
ensuring daily trial activities strictly follow the approved protocol, supporting accurate record-keeping,
and coordinating with monitors and investigators to address discrepancies quickly. Their ongoing oversight
is key to maintaining data quality and overall study integrity.
Phase 2: Study Conduct Phase
CRCs support active trial execution and ensure ongoing compliance throughout the conduct phase. CRCs also support the clinical research coordinator for job description by assisting with adverse event reporting and serious adverse event reporting in coordination with the investigator and sponsor.
Patient Visit Coordination and Study Activities
The CRC coordinates participant visits according to the study schedule by arranging appointments, preparing visit-related materials, and supporting site staff during study procedures. This helps ensure visits are conducted on time and in line with protocol requirements.
Informed Consent and Participant Support
CRCs support the informed consent process and informed consent documentation, ensuring ethical participation and compliance. The CRC also assists with participant communication to support adherence to visit schedules and study requirements.
Data Collection and Documentation Maintenance
CRCs maintain source documentation, complete case report forms, and support data entry and data accuracy. This helps maintain data quality and consistency throughout the study.
Monitoring Visit and Sponsor Coordination
CRCs support monitoring visit support, SDV activities, and maintain audit and inspection of readiness, ensuring study documents are available for review, and addressing follow-up actions. This helps maintain ongoing oversight and inspection of readiness during the study.
CRC Responsibilities During the Study conduct Phase
CRC Activity
Purpose
What It Ensures
Patient visit coordination and study activities
Manage scheduled study visits and protocol-required procedures
Protocol-compliant and timely study visits
Informed consent and participant support
Maintain valid, informed, and ongoing consent
Ethical participant involvement and regulatory compliance
Data collection and documentation maintenance
Record, verify, and manage study data accurately
Data quality, traceability, and consistency
Monitoring visit and sponsor coordination
Support sponsor monitoring, audits, and oversight activities
Inspection readiness and timely issue resolution
What Happened
Impact
Why CRC Matters
During the conduct phase of clinical trials, loss to follow-up occurs when enrolled participants fail to
return for scheduled study visits or withdraw prematurely. Clinical research methods literature indicates
that approximately 20% of subjects may be lost to follow-up, which can introduce bias and misleading
results, particularly when missing outcomes differ between treatment groups.
High rates of loss to follow-up can distort treatment effect estimates, threaten the internal validity of
trial results, and necessitate additional statistical adjustments or sensitivity analyses. These issues
complicate data interpretation and may raise concerns during regulatory review and acceptance.
Clinical Research Coordinators (CRCs) play a key role in minimizing loss to follow-up by maintaining
participant engagement, proactively tracking visit schedules, following up with participants, and
documenting reasons for missed visits. Their efforts help protect data completeness, reduce bias, and
preserve the overall quality and validity of trial data.
Phase 3: Study Close-Out Phase
The study close-out phase begins after the last participant completes the final study visit and continues until all study activities at the site are formally completed. During this stage, the Clinical Research Coordinator (CRC) supports the completion of site-level activities by ensuring documentation is finalized, data is resolved, and the site is ready for study closure and potential inspections.
Final Patient Visit and Study Completion Support
The CRC supports final study visits by coordinating end-of-study assessments, ensuring required procedures are completed, and confirming that participant records are properly closed. This helps ensure that all subject-related activities are completed in line with the protocol.
Data Cleaning and Query Resolution
During close-out, the CRC supports data cleaning by responding to outstanding data queries, verifying source documents, and assisting with final Case Report Form (CRF) completion. This helps ensure that data is accurate, complete, and ready for database locking.
Essential Document Review and Archival Preparation
The CRC reviews the Investigator Site File (ISF) to ensure all required documents are complete, current, and properly filed. This includes confirming approvals, correspondence, and study records are ready for long-term storage according to regulatory requirements ensure records meet essential documents of maintenance standards.
Close-Out Visit and Sponsor Coordination
The CRC supports site close-out visits by coordinating with Clinical Research Associates (CRAs), making documents available for review, and addressing close-out findings. This helps ensure that all site responsibilities are formally completed and documented.
CRC Responsibilities During the Study Close-Out Phase
CRC Activity
Purpose
What It Ensures
Final patient visit coordination
Support completion of end-of-study and follow-up visits
Proper subject closure in accordance with the protocol
Data cleaning and query resolution
Address outstanding data issues and resolve queries
Readiness for database lock and analysis
Essential document review (ISF)
Verify completeness and accuracy of study documentation
Inspection-ready study records
Close-out visit support and coordination
Assist the CRA during site close-out activities
Formal completion of site-level study activities
What Happened
Impact
Why CRC Matters
The U.S. FDA issued a warning letter to a clinical investigator for failing to retain required study records
for the mandated retention period. Record retention is a critical responsibility during the study
close-out and archiving phase, and failure to meet these requirements represents a significant regulatory
non-compliance.
Inadequate or missing record retention raises serious concerns regarding the validity, reliability, and
integrity of site-level trial data. Such deficiencies can result in corrective and preventive actions
(CAPAs), heightened regulatory scrutiny, and potential restrictions on future research activities.
During the close-out phase, Clinical Research Coordinators (CRCs) help prevent record retention failures by
reconciling essential documents, ensuring proper archiving, maintaining document traceability, and
confirming that records remain accessible for inspections throughout the required retention period. Their
oversight helps keep the site inspection-ready even after trial completion.
Skills Required for a Clinical Research Coordinator (CRC)
A Clinical Research Coordinator requires a strong foundation in clinical research and technical skills to support compliant trial execution. This includes understanding clinical trial protocols, ICH-GCP compliance, informed consent handling, source data verification, and proper management of essential study documents such as the Investigator Site File (ISF). These skills ensure trials are conducted ethically, data remains accurate, and sites remain inspection-ready throughout the study’s lifecycle.
In addition to technical knowledge, CRCs need operational and professional skills to manage daily trial activities effectively. This includes coordinating study visits, working closely with investigators, CRAs, and study teams, resolving data queries, tracking timelines, and maintaining clear communication. Strong attention to detail, time management, and ethical awareness enable CRCs to handle multiple responsibilities while maintaining compliance and consistent trial performance.
Conclusion
A CRC’s daily work directly affects trial quality, patient safety, and data integrity. From documentation to coordination, clinical research coordinator roles and responsibilities are central to ethical and efficient research execution. Every task, whether managing patient visits, maintaining documentation, or supporting compliance, directly affects the quality, safety, and credibility of a clinical trial. This makes the CRC role essential to ensuring that research studies are conducted responsibly and efficiently at the site level.
For those exploring a career in clinical research, understanding the CRC role provides clarity on what real trial execution looks like beyond theory. To learn more about this role in depth, explore the skills that define the CRC blogon the CliniLaunch website, and for hands-on, job-ready training, consider enrolling in the Advanced Diploma in Clinical Research to build the skills required to succeed in this field.
FAQ
1. What are the roles and responsibilities of a Clinical Research Coordinator?
A Clinical Research Coordinator supports the day-to-day conduct of clinical trials at the site. They coordinate study activities, manage documentation, support patient visits, and ensure the trial follows the approved protocol and GCP requirements.
2. What does a Clinical Research Coordinator do in a clinical trial?
A CRC coordinates patient visits, maintains study records, supports data entry, and works with investigators and monitors to keep the trial running smoothly and compliantly throughout its lifecycle.
3. What is the difference between a CRC and a CRA?
A CRC works at the study site handling daily trial execution, while a CRA works for the sponsor or CRO to monitor sites, review data, and ensure compliance across multiple sites.
4. What is the difference between a CRC and a CRA?
A CRC typically reports to the Principal Investigator (PI) at the site and works closely with Clinical Research Associates (CRAs) for study of coordination and monitoring activities.
5. What qualifications are required to become a Clinical Research Coordinator?
Most CRCs have a background in life sciences, pharmacy, nursing, or healthcare. Formal training in clinical research and GCP knowledge significantly improves eligibility and readiness for the role.
6. What skills are needed for a Clinical Research Coordinator?
CRCs need strong protocol understanding, documentation skills, attention to detail, coordination ability, and clear communication skills to manage study activities and compliance effectively.
7. What is the role of a CRC in patient safety?
CRCs support patient safety by ensuring informed consent is properly documented; adverse events are reported on time, and study procedures are followed as per protocol and ethical guidelines.
8 . Does a Clinical Research Coordinator take informed consent?
A CRC supports the informed consent process by explaining study details and documenting consent, but the investigator retains final responsibility for ensuring consent is ethically and medically appropriate.
9. Is Clinical Research Coordinator a good career option?
Yes, the CRC role offers hands-on exposure to clinical trials, strong demand across hospitals and research sites, and a solid foundation for long-term growth in clinical research.
10 . What is the career growth path for a Clinical Research Coordinator?
With experience, CRCs can progress to roles such as Senior CRC, CRA, Clinical Trial Manager, or Project Coordinator, depending on skills, exposure, and career interests.
A Clinical Data Coordinator supports clinical trials by reviewing and coordinating study data to ensure it is accurate, consistent, and inspection-ready.
This role covers data review, query coordination, safety data alignment, documentation support, and database lock readiness across the trial lifecycle.
The Clinical Data Coordinator is one of the most critical entry-level roles in clinical research for anyone aiming to build a non-laboratory career in healthcare. As clinical trials become increasingly data-driven, multi-site, and tightly regulated, this role exists to protect one thing the industry cannot afford to lose: data integrity.
Every clinical trial generates massive volumes of patient data. That data must be accurate, consistent, traceable, and compliant with global regulatory standards. If it is not, the trial risks delays, audit findings, inspection observations, or outright failure. The clinical data coordinator plays a central role in preventing those outcomes by ensuring trial data is review-ready, compliant, and reliable throughout the study lifecycle.
For students exploring a career in clinical research, understanding this role is often the first practical step toward entering the industry without working at the lab bench.
Who is a Clinical Data Coordinator?
A Clinical Data Coordinator (CDC) is a clinical research professional who supports clinical data management activities during a clinical trial. This role does not generate patient data. Instead, it focuses on reviewing, validating, and coordinating data collected from clinical sites to ensure it meets protocol, quality, and regulatory requirements.
CDC works closely with clinical research associates, investigators, site teams, and data managers. Their job is to make sure data entered into electronic data capture systems is accurate, complete, consistent, and aligned with the study protocol.
In practical terms, this role sits between data collection at the site level and centralized data management. By coordinating data flow across teams and systems, the clinical data coordinator ensures that issues are identified early, queries are handled properly, and patient safety data remains consistent across the trial.
For beginners, this role offers structured exposure to how real clinical trials operate from a data quality, compliance, and regulatory perspective, making it a common and logical entry point into clinical research careers.
Core Responsibilities of a Clinical Data Coordinator
The core responsibilities of a Clinical Data Coordinator focus on ensuring that clinical trial data is accurate, complete, traceable, and compliant throughout the study lifecycle. This role supports the smooth flow of data from clinical sites to central databases while maintaining regulatory alignment and database readiness.
Below is a clear and beginner-friendly explanation of clinical data coordinator roles and responsibilities, supported by real-world, industry-based examples.
1.Supporting Clinical Data Management Activities
Clinical trials follow a predefined data management plan that defines how data should be collected, reviewed, cleaned, and locked. The Clinical Data Coordinator supports this plan by ensuring that daily data workflows are executed consistently across the study. This includes coordinating data review cycles, tracking data-related issues, and working closely with central data management teams to resolve inconsistencies early rather than at the end of the trial.
2.Case Report Forms and eCRF Handling
Case report forms are the primary tools used to capture patient data in a clinical trial. In most modern studies, this data is entered through electronic case report forms using electronic data capture systems. The Clinical Data Coordinator ensures that these forms are completed accurately and in line with the approved protocol. This involves reviewing form completeness, verifying required fields, coordinating updates after protocol amendments, and supporting corrections when inconsistencies are identified. Proper CRF and eCRF handling are essential for maintaining data consistency and accuracy across study sites.
Advanced Diploma in
Clinical Research
Build practical, industry-aligned skills to work across real clinical trial environments. Learn how clinical studies are planned, conducted, documented, and monitored, with a strong emphasis on ethics, patient safety, and regulatory compliance throughout the trial lifecycle.
Although patient data is entered by clinical sites, the Clinical Data Coordinator plays a key role in reviewing and validating that data before it progresses through the data lifecycle. This includes checking entries in electronic data capture systems for missing, illogical, or inconsistent values and supporting structured data entry and validation of workflows. When recurring issues are identified, they are escalated to data managers to prevent systemic data quality problems. These activities contribute directly to early-stage data cleaning in clinical trials.
4.Query Management and Data Cleaning
When discrepancies or missing information are identified during data review, data queries are raised for clarification. The Clinical Data Coordinator supports query management by reviewing system-generated and manual queries, coordinating responses with site teams, and tracking query resolution status. Active involvement in ongoing data cleaning helps prevent query backlogs and reduces delays during database locks.
Real-Life Case Study: How Query Backlogs Delay Database Lock
In a multi-site Phase III clinical trial, data queries were raised regularly for missing and inconsistent entries, but follow-ups with sites were delayed. As the study approached database lock, unresolved queries accumulated, slowing final data cleaning and putting the lock timeline at risk.
The Clinical Data Coordinator intervened by prioritizing high-impact queries, coordinating closely with sites and Clinical Research Associates, and enforcing structured tracking with clear timelines. This focused approach cleared the backlog, enabled database lock on schedule, and prevented delays to final analysis and regulatory activities.
Regulatory guidance from the U.S. FDA emphasizes timely data review, correction of discrepancies, and readiness of electronic source data before database lock and submission.
5.Source Data Verification Support
During monitoring visits, Clinical Research Associates perform source data verification by comparing site source documents with data entered the clinical database. The Clinical Data Coordinator supports this process by clarifying discrepancies raised during monitoring, coordinating corrections with sites, and ensuring related documentation is updated correctly. This support strengthens audit and inspection of readiness and improves overall trial quality.
6. Patient Safety Data Coordination
Patient safety data must be accurate, timely, and consistent across systems to meet regulatory expectations. The Clinical Data Coordinator supports patient safety data coordination by verifying adverse event entries, ensuring consistency between safety databases and case report forms, escalating missing or delayed safety data, and aligning safety information with regulatory reporting timelines.
Real-Life Case Study: Inconsistent Patient Safety Data Across Systems
During routine data review in an ongoing clinical trial, inconsistencies were identified between adverse events recorded in case report forms and entries in the safety database. If left unresolved, these discrepancies could have resulted in compliance findings during regulatory inspection.
The Clinical Data Coordinator reviewed safety data entries, coordinated corrections with study sites, and ensured alignment between clinical and safety systems. As a result, patient safety data became consistent across platforms; regulatory reporting timelines were met, and inspection risk was reduced.
Regulatory inspection trend reports published by the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) frequently cite safety data inconsistencies and documentation gaps as inspection observations.
7. Regulatory Compliance and ICH GCP Alignment
All clinical trial data activities must align with ICH GCP compliance and applicable regulatory requirements. The Clinical Data Coordinator ensures protocol adherence during data review, proper documentation for audits, and compliance with regulatory expectations. The coordinator also supports sponsor reviews and inspections by maintaining inspection-ready data and documentation throughout the trial.
8.Trial Master File and Documentation Support
Proper documentation is essential for trial transparency and regulatory inspections. The Clinical Data Coordinator supports trial master file activities by ensuring that data-related documents are filed correctly, version control is maintained, and documentation practices remain inspection-ready throughout the study.
Real-Life Case Study: Preventing Audit Findings Through Proper Documentation
During a sponsor audit, missing data review documentation was identified for several completed study visits. Although the clinical data itself was accurate, incomplete documentation raised concerns about data traceability and inspection readiness.
The Clinical Data Coordinator reviewed filing practices, ensured missing documents were added to the trial master file, and standardized documentation workflows. The audit observations were resolved successfully, and improved documentation practices were applied to ongoing and future studies.
Regulatory inspection summaries published by the U.S. Food and Drug Administration (FDA) consistently highlight documentation gaps and incomplete records as common audit findings in clinical trials.
9.Database Lock Support
Before a clinical trial database can be locked, all data queries must be resolved, and final data reviews completed. The Clinical Data Coordinator supports database lock activities by tracking outstanding queries, confirming site responses, supporting final review cycles, and coordinating with data managers prior to lock approval. This ensures that the database is complete, accurate, and ready for submission.
10.Medical Coding Coordination
Some clinical trials require standardized coding of medical terms such as adverse events and medications. The Clinical Data Coordinator assists in medical coding coordination by supporting review of coded terms, coordinating corrections when inconsistencies are identified, and ensuring consistency across datasets used for analysis and reporting.
11. Collaboration with Clinical Teams
Clinical trials depend on effective coordination across multiple teams. The Clinical Data Coordinator works closely with Clinical Research Associates, investigators, site staff, and data managers to resolve data-related issues, support site communication, and ensure smooth operational flow throughout the trial.
Together, these responsibilities ensure that clinical trial data is reliable, audit-ready, and suitable for regulatory submission, reinforcing the Clinical Data Coordinator’s role as a critical link between clinical sites and data management teams.
Key Skills and Career Growth for a Clinical Data Coordinator
Key Skill Area
What It Enables in the Role
How This Skill Is Built
Career Growth It Supports
Attention to Detail & Data Review
Identifying missing, inconsistent, or incorrect data
Regular data review, query checks, and CRF verification
Progression to Senior Clinical Data Coordinator
Clinical Data Management Knowledge
Working with CRFs, eCRFs, and data review cycles
Exposure to data management plans and review workflows
Transition into Clinical Data Analyst or Data Manager
Regulatory & ICH GCP Awareness
Ensuring compliant data handling and audit readiness
Working with protocols, GCP guidelines, and inspections
Eligibility for lead and compliance-focused roles
Query Management & Issue Resolution
Coordinating with sites and CRAs to close data queries
Handling live queries and site clarifications
Study-level ownership and senior coordinator roles
Problem-Solving Ability
Identifying data issues and driving corrective actions
Managing discrepancies and recurring data issues
Readiness for complex trials and lead roles
Communication & Coordination
Working with investigators, CRAs, and data teams
Daily interaction with cross-functional teams
Growth into Clinical Data Operations roles
Documentation & Process Tracking
Maintaining inspection-ready records
Managing trackers, TMF documents, and audit files
Supports management and oversight responsibilities
Advanced Diploma in
Clinical SAS
Build practical skills in clinical data analysis and statistical reporting using SAS, aligned with regulatory standards used in clinical trials. Learn how clinical trial data is structured, analyzed, and converted into submission-ready outputs.
The Clinical Data Coordinator role exists to keep a clinical trial under control. Modern trials involve multiple sites, large volumes of patient data, and strict regulatory oversight. When data is not reviewed, coordinated, and resolved in real time, problems surface late, during audits, inspections, or database lock. This role prevents that by acting as the link between sites, clinical teams, and data management.
For beginners, the value of this role is exposure. You see how trials actually function, how data flows, where mistakes happen, and how those mistakes are corrected before they become regulatory issues. You are not isolated in one task; you are embedded in the operational backbone of a trial.
To enter and succeed in this role, theoretical knowledge alone is not enough. What matters is practical familiarity with clinical trial workflows and regulatory expectations. Structured, industry-aligned training helps bridge that gap and prepares candidates to operate confidently in real clinical research environments.
Clini Launch Research Institute offers an industry-aligned clinical research course that equips learners with the skills and hands-on exposure required to confidently begin a career as a Clinical Data Coordinator and grow within the clinical research industry.
FAQs
1. What does a Clinical Data Coordinator do?
A Clinical Data Coordinator reviews and coordinates clinical trial data to ensure it is accurate, complete, and compliant with study protocols and regulatory guidelines.
2. Is the Clinical Data Coordinator role suitable for beginners?
Yes. It is an entry-level role in clinical research and is suitable for life science graduates who want a non-laboratory career path.
3. Does a Clinical Data Coordinator perform data entry?
No. Data is entered by clinical sites. The coordinator reviews, validates, and resolves data issues.
4. What tools does a Clinical Data Coordinator work with?
They commonly work with electronic data capture systems, clinical trial management systems, safety databases, and trial master file systems.
5. What is the career growth after becoming a Clinical Data Coordinator?
With experience, professionals can progress into Senior Clinical Data Coordinator, Clinical Data Manager, or Clinical Data Operations roles.
6. How can I prepare for a Clinical Data Coordinator role?
Preparation involves understanding clinical research processes, basic data management concepts, regulatory guidelines, and gaining practical exposure through structured training.
Informed Consent in Clinical Trials
Informed consent in clinical trials is an ongoing process where participants are clearly informed about the study purpose, procedures, potential risks, expected benefits, and their right to withdraw from the study at any time without penalty.
Every clinical trial begins with a single non-negotiable requirement: informed consent. Before a participant can be screened, tested, or exposed to any study-related procedure, their voluntary and informed agreement must be obtained and documented. This is not an administrative formality. It is the ethical and legal foundation of clinical research.
Without valid informed consent, a clinical trial cannot proceed, no matter how well designed the protocol is or how promising the investigational treatment may be. Failures in the consent process have repeatedly led to trial suspensions, regulatory action, and loss of public trust. This is why informed consent is treated as a core ethical responsibility in clinical research, not just a signed document.
What Is Informed Consent in Clinical Trials
In clinical trials, the informed consent process means that a participant clearly understands what a study involves and agrees to take part voluntarily. Before joining a trial, the participant is informed about the study’s purpose, what procedures will take place, the possible risks and benefits, and their right to refuse or withdraw at any time. Only after this information is clearly understood can a participant make an informed decision to participate.
In simple terms, this explains the informed consent process and how it is applied in real clinical trial settings as an ongoing communication process rather than just a signed form.
Informed Consent Is a Process, not a Signature
Many people think informed consent is just signing a form. This is not true. Informed consent is an ongoing process. It starts when the study is first explained and continues throughout the trial. Participants should always be kept informed. If anything changes in the study or new risks are found, the participant must be told again and given a chance to decide whether they still want to continue.
The 3 Core Requirements of Informed Consent
For informed consent to be valid in a clinical trial, it must meet three essential requirements. If even one of these is missing, the consent is considered incomplete. These requirements are central to the informed consent definition used in ethical clinical research.
1. Voluntary
Consent must be given freely and without pressure. The participant should never feel forced, rushed, or afraid to say no.
This means:
Participation is optional
Saying no will not affect medical care
The participant can leave the study at any time
For example, a participant should not feel that joining the trial is the only way to receive treatment or medical attention. True consent exists only when the decision is made by choice.
2. Understandable
The information shared must be easy to understand. Using complex medical terms or speaking too fast can prevent real understanding.
This means:
Information should be explained in simple language
Medical jargon should be avoided or clearly explained
The participant should be encouraged to ask questions
Understanding is not assumed just because someone signs a form. Researchers must make sure the participants truly understand what the study involves.
3. Informed
The participants must receive complete and honest information about the study.
This includes:
Why the study is being done
What will happen during the study
Possible risks and side effects
Possible benefits (or lack of direct benefit)
Other treatment options available
Consent is considered informed only when the participant has enough information to make a thoughtful and confident decision.
Advanced Diploma in
Clinical Research
Build industry-ready skills to work across real clinical trial environments, from study initiation to close-out. Learn how clinical research actually operates in hospitals, CROs, pharma companies, and research organizations, with a strong focus on compliance, documentation, and trial execution.
What Participants Must Be Told During Informed Consent
For informed consent to be valid, participants must be clearly told about certain essential information before they agree to join a clinical trial. This ensures they can decide with confidence, clarity, and without pressure.
Purpose, Duration, and What Will Happen
Participants must be told:
Why the study is being done and what question it aims to answer
How long the study will last, including follow-up periods
What exactly will happen to them, such as clinic visits, tests, treatments, or sample collection
This helps participants understand the level of involvement required and decide whether the study fits their personal and medical situation.
Risks, Discomforts, and Possible Benefits
Participants must be informed about:
Possible risks and side effects, even if they are uncommon
Any physical, emotional, or practical discomfort they may experience
Possible benefits, if any, and whether there may be no direct benefit to them
Risks must be explained honestly and clearly so participants can balance potential harm against possible benefits before deciding.
Alternatives to Participation
Participants must be told:
Other available treatment or care options
That choosing not to participate will not affect their access to medical care
This ensures participants do not feel pressured to join the study or believe it is their only option.
Privacy, Confidentiality, and Data Use
Participants must understand:
How their personal and medical information will be collected and stored
Who may access their data, such as researchers or regulatory authorities
How their identity will be protected as far as possible
These build trust and reassure participants that their personal information will be handled responsibly.
Costs, Compensation, and Treatment for Injury
Participants must be told:
Whether there are any costs related to participating in the study
If compensation or reimbursement is provided for time or travel
What medical care or compensation is available if a study-related injury occurs
Clear communication in this area helps prevent confusion or disputes later.
Right to Refuse or Withdraw Without Penalty
Participants must be clearly told that:
Participation in the study is completely voluntary
They can refuse to participate without giving a reason
They can withdraw from the study at any time without losing medical care or benefits
This reinforces participant’s autonomy and ensures they remain in control of their decision.
Whom to Contact for Questions and Emergencies
Participants must be given:
Contact details of the study investigator or study team
Information on whom to contact for general questions
Emergency contact details for urgent situations
This ensures participants know where to seek help or clarification at any stage of the study.
How the Consent Process Works in Real Clinical Trials
In real clinical trials, informed consent is not a one-time formality. It is a structured, step-by-step process designed to protect participants before they join a study and while the study is ongoing. Regulatory authorities such as the U.S. Food and Drug Administration clearly state that informed consent must be obtained before any study-related activity begins and must continue throughout the trial. This section shows informed consent processes in real clinical trials, beyond theory and documentation.
1. When Consent Happens — Before Any Study Procedure
In clinical trials, informed consent must be obtained before:
Any screening tests
Any study-related examination
Any trial medication or intervention
Any data or sample collection
The study team explains the study in detail, answers questions, and ensures the participant understands the information. Only after this discussion does the participant sign the informed consent form. If any study procedure happens before consent, the consent is considered invalid.
When Consent Comes Too Late: India’s 2010 Clinical Trial Crisis
In the early 2010s, serious concerns emerged in India regarding how clinical trials were conducted. Reports indicated that some participants were enrolled without fully understanding the study, and in certain cases, informed consent was obtained only after study-related procedures had already begun.
These concerns reached the Supreme Court of India through a public interest litigation filed by Swasthya Adhikar Manch, an organization advocating for patient rights. The court examined whether trial participants were adequately informed before being exposed to investigational drugs or procedures.
The findings were significant. In 2013, the Supreme Court halted approvals for new clinical trials until stricter safeguards were established. A key issue identified was the failure to obtain valid informed consent prior to any study procedure.
This case reinforced a fundamental principle of clinical research: consent obtained after a procedure is not considered valid informed consent.
The outcome reshaped India’s clinical trial oversight framework and demonstrated how failures in informed consent can lead to major legal and regulatory intervention.
2. “Key Information” Upfront — What Matters Most First
In real consent discussions, participants are first given key information that directly affects their decision, such as:
Why the study is being conducted
What will happen to them
Major risks and possible benefits
The voluntary nature of participation
This information is presented before lengthy technical details, so participants can quickly understand what truly matters and decide whether they want to continue learning about the study.
When Key Information Is Not Told First: The Coventry Chapati Study
Another important lesson in informed consent comes from the United Kingdom. In a nutrition study conducted in Coventry, South Asian women were given chapatis containing a radioactive iron isotope to examine iron absorption. Although consent documentation existed, later reviews identified a serious ethical failure.
Many participants were not clearly informed at the outset that radioactive material was involved. The true nature of the study and its potential risks were not explained in a manner the participants could easily understand. Critical information was either minimized or not communicated clearly at the beginning of the consent process.
This study later became widely cited in bioethics discussions because it demonstrated that informed consent fails when key information is hidden, delayed, or deprioritized—even if a consent form is signed.
The Coventry Chapati Study reinforced a fundamental principle of ethical research: participants must receive the most important information first—study purpose, procedures, and risks—before secondary details or paperwork.
The case continues to be referenced as a clear example of why transparency at the very start of the informed consent process is essential.
3. Ongoing Consent During the Study
Informed consent does not end once the form is signed. During the study:
Participants may ask questions at any time
New risks or safety findings must be shared
Protocol changes may require re-consent
Participants must be free to reconsider and withdraw
This ensures that consent remains informed and voluntary throughout the study, not just at the beginning.
When Consent Is Treated as a One-Time Event: HIV Trials in Uganda
A different type of informed consent failure was observed in HIV clinical trials conducted in Uganda. In these studies, participants signed informed consent forms correctly at the time of enrollment, and on paper, the consent process appeared compliant with regulatory requirements.
However, follow-up assessments of participant understanding revealed significant gaps over time. Many participants did not fully understand the study as it progressed. Some were unclear about their right to withdraw, while others misunderstood ongoing study procedures and expectations.
Contributing factors included language barriers, low literacy levels, and long study durations. Without repeated explanations and reinforcement, participant understanding gradually declined. Researchers concluded that a single consent discussion at the beginning of the trial was insufficient.
This led to an important principle in modern clinical research: informed consent is an ongoing process. Participants must be given continuous opportunities to ask questions, receive updates, and reconfirm their willingness to participate—especially when new information or changes arise during the study.
Documentation and Formats in the Informed Consent Process
In clinical trials, informed consent must be documented properly to show that a participant understood the study and agreed to take part before any study procedure began. Proper documentation supports the informed consent form and compliance with ethics committee (IEC/IRB) requirements.
1.Written Consent and Signatures
The study is explained to the participant
The informed consent form is signed and dated
The investigator also signs the form
This signed document is the official proof of consent. It confirms that consent was taken correctly and on time.
2.Witness or Translator (When needed)
Used when a participant cannot read or understand the consent form
A translator explains the study in the participant’s language
A witness confirms the explanation and signs
This ensures that consent is truly understood. It protects participants from agreeing without understanding.
3.Electronic Informed Consent (eConsent)
Consent is taken digitally using a tablet or computer
May include videos or simple explanations
Digital signatures and timestamps are recorded
This helps reduce paperwork errors and improves understanding. It makes the consent process clearer and more reliable.
Advanced Diploma in
Medical Coding
Develop skills in clinical documentation, medical records analysis, and compliance practices that support ethical patient care and informed consent processes across healthcare and research settings. This program focuses on accuracy, standards, and real-world documentation workflows.
Special Situations Beginners Must Know in Informed Consent
In real clinical trials, informed consent does not always happen in a simple situation where an adult participant reads a form and signs it. Certain special situations require extra care to protect participants and ensure that consent remains ethical, valid, and fair.
1.Legally Authorized Representative (When a Participant Can’t Consent)
Sometimes, a participant is unable to give informed consent on their own, such as:
When the participant is unconscious
When there is severe cognitive impairment
When the participant is critically ill
In these situations, consent is obtained from a Legally Authorized Representative (LAR) usually a close family member or legal guardian, as permitted by law. Guidance from the U.S. Department of Health and Human Services makes it clear that this option is used only when the participant truly cannot decide for themselves.
The LAR is expected to act in the best interest of the participant, not for convenience or speed.
2.Assent for Minors
Children cannot legally provide informed consent on their own. When clinical research involves minors:
Consent must be obtained from a parent or legal guardian
The child’s assent (agreement) should also be sought, when appropriate
Assent means explaining the study to the child in age-appropriate, simple language and respecting their willingness or refusal to participate. Ethical guidance from the U.S. Department of Health and Human Services emphasizes that children should be involved in the decision as much as they are able to understand.
3.Vulnerable Participants and Undue Influence
Some participants may be considered vulnerable, such as:
Economically disadvantaged individuals
Patients’ dependent on doctors, caregivers, or institutions
Individuals with limited education or low health literacy
In these cases, extra safeguards are required to ensure participation is truly voluntary. Guidance from the U.S. Food and Drug Administration stresses that consent must not be influenced by fear, authority, financial pressure, or promises of better care.
Participants must clearly understand that saying “no” will not affect their treatment or benefits.
4.Waiver, Alteration, and Emergency Exceptions (High-Level)
In rare situations, informed consent requirements may be waived or altered, such as:
Certain minimal-risk research
Emergency situations where immediate medical action is required
These exceptions are strictly controlled and allowed only with ethics committee approval and under regulations outlined in the eCFR. Consent is not ignored; it is adjusted only when participant’s safety or urgent public health needs require it.
5.Re-Consent After Protocol Changes or New Risk Information
Informed consent is an ongoing process, not a one-time event. If:
The study protocol changes
New risks are identified
New information affects participant safety
Participants must be informed again, and re-consent may be required. Guidance from the ICH makes it clear that participants have the right to reconsider their participation when new information emerges.
Key Takeaway for Beginners
Informed consent is about protecting people, not paperwork.
Even in special or complex situations, consent is never skipped. Instead, it is adapted to ensure fairness, understanding, and respect. This may involve consent from a legally authorized representative, support through a child’s assent, additional safeguards for vulnerable participants, adjustments in emergency settings, or repeating consent after study changes.
Regardless of the situation, the objective remains the same: participants must always have a meaningful choice about whether to take part in the research.
Common Consent Mistakes (And Why They’re Serious)
In clinical research, informed consent usually fails not because of bad intent, but because of small, routine mistakes. For beginners, it’s important to recognize these mistakes early, because even simple errors can make consent ethically invalid and create serious regulatory issues. Many of these mistakes arise from misunderstanding the difference between consent and informed consent.
Using “Too Technical” Language and Poor Understanding
One of the most common consent mistakes is explaining the study using complex medical or scientific language that participants cannot easily understand.
This typically happens when:
Consent forms are written like scientific or regulatory documents
Medical terms are not explained in simple language
The study is explained quickly without checking understanding
Regulatory expectations under the eCFR require that consent information be understandable to the participant. If a participant does not truly understand what they are agreeing to, the consent is not considered informed even if the form has been signed.
Coercion, Pressure, or Misleading Promises
Another serious mistake is influencing participants through pressure, authority, or misleading information, rather than allowing them to decide freely.
This can occur when:
Doctors or study staff unintentionally pressure participants
Participants fear losing medical care if they refuse
Benefits are exaggerated or described as guaranteed
Guidance from the U.S. Food and Drug Administration clearly states that informed consent must be voluntary and free from coercion or undue influence. If a participant agrees because they feel pressured or misled, the consent is no longer voluntary and therefore not valid.
Missing Key Elements or Using the Wrong Consent Version
Consent can also fail due to documentation and version-control errors, even when the study has been explained properly.
Common examples include:
Missing participant or investigator signatures
Missing dates on the consent form
Use of an outdated or unapproved consent version
Regulations require that only the current, ethics committee approved consent form is used. Even when participant’s understanding is adequate, incorrect or incomplete documentation can lead to serious findings during audits and may invalidate the participant’s consent.
Roles Where Consent Knowledge Is Non-Negotiable
In clinical research, informed consent is not handled by a single role. Different professionals interact with the consent process at different stages of a trial. For some roles, consent knowledge is part of daily responsibilities; for others, it is essential for verification, documentation, and oversight. In all cases, gaps in consent understanding can lead to ethical and compliance issues.
Role
How the Role Interacts with Informed Consent
Clinical Research Coordinator (CRC)
Explains the study to participants, ensures the correct consent version is used, confirms that informed consent is obtained before any study procedure, and manages re-consent when required.
Clinical Research Associate (CRA)
Reviews informed consent forms during monitoring visits, checks signatures, dates, and version control, and verifies that consent was obtained before study-related procedures.
Research Nurse
Supports consent discussions with clinical explanations, identifies participant confusion or concerns, and flags situations where re-consent may be necessary.
Clinical Trial Assistant (CTA)
Maintains and files informed consent documents, tracks approved consent versions, and supports audits and inspections related to consent records.
Why This Matters Across All Roles
Informed consent failures are rarely caused by one individual. A single consent issue often results from multiple small gaps across roles incomplete explanations, missed checks, or documentation errors. When consent knowledge is shared and understood across the team, participant rights are better protected and trial integrity is maintained.
Conclusion
Informed consent is where ethical intent is tested in real clinical practice. It is the point at which regulations, human judgment, communication skills, and accountability intersect. When handled correctly, it protects participants and preserves the credibility of the research. When handled poorly, it exposes trials to ethical failure, regulatory action, and lasting damage to public trust.
For anyone entering clinical research, informed consent is not just a topic to understand, but a responsibility to uphold. It shapes how studies are conducted, how participants are treated, and how confidently a trial can stand up to scrutiny. This is why we at CliniLaunch Research Institute treat this as a foundational competency in our clinical research training programs and not as a procedural checklist.
Learning the informed consent process early builds the mindset required for ethical decision-making, regulatory compliance, and participant-centered research—skills that define competent clinical research professionals across roles and settings.
FAQs
1. What is the informed consent process in clinical research? The informed consent process is an ongoing communication process where participants are informed about a study and voluntarily decide whether to take part.
2. What is the difference between consent and informed consent? Consent is simply agreeing, while informed consent means agreeing after fully understanding the study, risks, benefits, and participant rights.
3. Who is responsible for obtaining informed consent in a clinical trial? Informed consent is usually obtained by the investigator or trained study staff responsible for explaining the study to participants.
4. Is informed consent a one-time signature or an ongoing process? Informed consent is an ongoing process that continues throughout the study, especially when new information or risks arise.
5. What information must be included in an informed consent form? An informed consent form includes study purpose, procedures, risks, benefits, alternatives, privacy details, and the right to withdraw.
6. Can a participant withdraw from a clinical trial after giving consent? Yes, participants can withdraw from a clinical trial at any time without penalty or loss of medical care.
A clinical trial protocol is a structured plan that defines how a clinical study is designed, conducted, monitored, and analyzed. It outlines objectives, participant eligibility, study design, safety measures, and statistical methods to ensure ethical, reliable, and consistent trial execution.
Every clinical trial operates within a clinical trial protocol, even though most beginners only encounter it as a document to be followed. In reality, the protocol is what turns a research idea into a controlled, ethical, and measurable clinical study. Without it, trials would vary from site to site, decisions would be inconsistent, and patient safety would be difficult to protect.
For anyone entering clinical research, understanding how trials are structured is more important than memorizing regulations or job titles. The protocol sits at the center of that structure. It connects scientific objectives with real-world execution and ensures that everyone involved is working from the same plan.
This blog explains what a clinical trial protocol is, why it exists, and how it shapes the way clinical research is planned, conducted, and evaluated in practice.
What Is a Clinical Trial Protocol and Why It Exists
A clinical trial protocol is the written plan that explains how a clinical study will be carried out from start to finish. It defines what the study is trying to answer, who can participate, what procedures will be performed, how safety will be monitored, and how results will be analyzed.
Clinical trial protocols exist because clinical research cannot rely on informal decision-making. Studies involve human participants, medical interventions, and regulatory oversight. The protocol establishes clear rules before the trial begins so that actions taken during the study are consistent, justified, and defensible.
By setting these rules in advance, the protocol serves two critical purposes. First, it protects participants by defining eligibility criteria, visit schedules, and safety assessments. Second, it protects the scientific integrity of the study by ensuring that data is collected and analyzed in a structured and reliable way.
In practice, the clinical trial protocol acts as both a scientific blueprint and an operational guide, making it possible for clinical trials to be ethical, reproducible, and acceptable to regulators.
Who Uses a Clinical Trial Protocol
A clinical trial protocol is used by everyone involved in a clinical study:
Investigators and doctors use it to understand how the study should be conducted and how participants should be treated.
Clinical Research Coordinators (CRCs) follow the protocol to schedule visits, perform procedures, and collect data correctly.
Clinical Research Associates (CRAs) use it to check whether the trial is being conducted according to plan.
Data management and statistics teams rely on the protocol to know what data to collect and how it should be analyzed.
Ethics committees and regulators, such as the FDA and ICH-GCP, review the protocol to ensure the study is ethical, safe, and scientifically sound.
In simple terms, the protocol in clinical trials acts as a shared guidebook for all stakeholders.
What Is Included in a Clinical Trial Protocol?
A clinical trial protocol contains clearly defined sections that explain why a study is conducted, how it will be carried out, and how safety and results will be evaluated. Each section plays a specific role in ensuring that the trial is ethical, consistent, and scientifically reliable.
1. Trial Identification and Administrative Details
This is the identity card of the study. It includes the official study title, protocol number, trial phase, sponsor name, investigator details, and version history.
Why it matters: These details establish investigator responsibilities, trace accountability, and ensure that every site, auditor, and regulator is working from the same approved version. Any mismatch here is a compliance problem, not a clerical error.
2. Background and Scientific Rationale
This section answers a simple but brutal question: Why does this study deserve to exist?
It summarizes current medical knowledge, gaps in evidence, and limitations of existing treatments. The scientific rationale justifies exposing real humans to risk and effort. Without a solid rationale, the study fails both scientifically and ethically.
This is where a clinical trial protocol definition moves beyond theory and proves relevance with data and prior research.
For example, the AURORA cardiovascular outcomes trial was conducted because patients on long-term dialysis had high cardiovascular risk, yet there was insufficient evidence that statins reduced events in this population.
3. Study Objectives and Endpoints
Here, the protocol stops being philosophical and becomes measurable.
Objectives state what the study is trying to prove.
Endpoints define how that proof will be measured.
Primary and secondary endpoints are clearly separated to avoid post-hoc manipulation. This clarity protects the study from biased interpretation and supports regulatory compliance during review.
A weak endpoint definition is one of the fastest ways to kill a study’s credibility.
The study design and methodology section explains:
Trial type (randomized, controlled, open-label, etc.)
Treatment arms and comparators
Randomization and blinding methods
Duration and follow-up structure
Good clinical trial protocol design ensures results are scientifically valid and defensible. Poor design guarantees wasted time, money, and participants.
5. Study Population and Eligibility Criteria
This section defines who gets in and who stays out.
Clear inclusion and exclusion criteria protect participants and prevent noise in the data. They also directly affect how widely the results can be applied in real clinical practice.
Eligibility criteria are a core part of risk benefit assessment. Enrolling the wrong population can expose patients to unnecessary risk or dilute meaningful outcomes.
A well-written schedule ensures consistency across sites and supports accurate data collection and management. Ambiguity here leads to protocol deviations, not flexibility.
7. Safety Monitoring and Risk Management
This section defines how participant safety is actively protected, not just promised.
It explains:
Adverse event reporting
Serious adverse event escalation
Stopping rules and discontinuation criteria
Ongoing safety review processes
This is where ethical considerations in clinical trials meet legal obligation. Continuous safety monitoring is mandatory under global clinical trial protocol guidelines, especially for studies conducted under regulatory frameworks like INDs.
Without rigorous controls, even a perfectly designed trial becomes unusable. Regulators care as much about how data was collected as they do about the results themselves.
9. Statistical Considerations
This is where math prevents false conclusions.
The protocol defines:
Sample size calculation
Statistical tests and assumptions
Power (typically 80–90%)
Significance thresholds
Predefining statistics protects the study from selective analysis and supports transparent interpretation. Changing numbers later is not “optimization”; it’s a red flag.
For example, The WOSCOPS trial used predefined statistical power calculations to ensure sufficient participants were enrolled to detect meaningful treatment effects.
10. Ethical Considerations and Informed Consent
No participant enters a trial without this section being rock solid. The protocol explains the informed consent process, confidentiality safeguards, and participant rights. Consent is not a formality. It is an ongoing ethical obligation backed by global standards like ICH GCP. This section anchors the entire study in human protection, reinforcing that compliance exists to serve people, not paperwork.
Build industry-ready skills to work across real clinical trial environments, from study initiation to close-out. Learn how clinical research actually operates in hospitals, CROs, pharma companies, and research organizations, with a strong focus on compliance, documentation, and trial execution.
In a clinical trial, multiple documents are used at different stages of the study. While the clinical trial protocol sets the overall direction, other documents support communication, execution, analysis, and compliance. Understanding how these documents differ helps clarify who uses what and at which point in the trial.
Protocol vs Informed Consent Form (ICF)
The clinical trial protocol is a technical document created for scientific and regulatory review. It defines the study framework and governs how the trial must be conducted.
The Informed Consent Form exists to support participant decision-making. Its role is ethical rather than operational; it ensures participants understand the study before agreeing to take part.
Protocol vs Investigator Brochure (IB)
The protocol focuses on trial conduct, while the Investigator Brochure focuses on knowledge transfer. The IB equips investigators with background information needed to use the investigational product safely, but it does not dictate how the study itself is running.
Protocol vs Statistical Analysis Plan (SAP)
The protocol establishes the analytical intent of the study on what outcomes matter and why. The SAP translates that intent into executable statistical instructions, ensuring that analysis of decisions is locked before results are examined.
Protocol vs Case Report Forms (CRFs)
The protocol defines what should be observed in a participant. CRFs exist only to capture those observations in a structured, auditable way. If the protocol changes, CRFs must be updated to remain aligned.
Protocol Amendments vs Protocol Deviations
Amendments reflect controlled evolution of the study plan, while deviations represent exceptions that occur during real-world execution. Both are tracked to assess their impact on safety and data integrity under ICH Good Clinical Practice.
How These Documents Function in a Trial
Document
When It Is Used
Primary Owner
What It Enables
Clinical Trial Protocol
Before and throughout the trial
Sponsor
Regulatory approval and trial governance
Informed Consent Form (ICF)
Before participant enrollment
Investigator / IRB
Ethical enrollment of participants
Investigator Brochure (IB)
Before site initiation and during trial
Sponsor
Investigator training and product safety awareness
Statistical Analysis Plan (SAP)
Before database lock
Biostatistics team
Predefined, unbiased data analysis
Case Report Forms (CRFs)
During participant visits
Data management
Standardized data capture
Protocol Amendment
When trial design needs revision
Sponsor
Controlled updates to study conduct
Protocol Deviation
When protocol is not followed
Site / Monitor
Documentation of execution gaps
Understanding how protocols translate into statistical plans and analysis is essential for roles that work closely with trial data and reporting.
Advanced Diploma in
Clinical SAS
Build practical skills in clinical data analysis and reporting using SAS, aligned with regulatory standards used in clinical trials. Learn how clinical trial data is cleaned, analyzed, and presented for regulatory submissions and study reporting.
Common Misconceptions About Clinical Trial Protocols
People new to clinical research often misunderstand what a clinical trial protocol actually does. These misconceptions usually come from seeing the protocol as a static or purely regulatory document, rather than a practical guide used throughout a trial.
1. The protocol is just paperwork
Many believe the protocol exists only to satisfy regulators.
In reality, the protocol guides daily trial activities such as participant visits, safety assessments, dosing decisions, and data collection.
2. Once written, the protocol never changes
It’s commonly assumed that protocols are fixed and cannot be modified.
In practice, protocols can be updated through approved amendments when scientific, operational, or safety-related changes are needed.
3. Only regulators care about the protocol
Another misconception is that the protocol is relevant only during inspections.
In reality, investigators, Clinical Research Coordinators, monitors, data managers, and statisticians rely on the protocol to perform their roles consistently.
Case Study 1: When the Protocol Made the Call
During a clinical trial, a participant developed unexpected safety symptoms after dosing, leaving the site team unsure whether treatment should continue. Instead of relying on judgment, the team followed the clinical trial protocol, which had already defined stopping rules and reporting timelines. Treatment was discontinued and the event was reported as outlined in FDA IND safety reporting requirements.
4. Protocol deviations mean the study has failed
Deviations are often viewed as signs of poor-quality trials.
In real-world settings, deviations are expected. What matters is how they are documented, assessed, and managed.
5. Participants read the clinical trial protocol
Some assume participants are given the full protocol.
In reality, participants interact only with the Informed Consent Form, which explains the study in plain language. The protocol remains a technical document used by the research team.
6. The protocol and SOPs are the same
Protocols and Standard Operating Procedures are often confused.
SOPs describe how an organization operates in general, while the protocol defines how one specific clinical trial must be conducted.
Case Study 2: A Missed Visit That Didn’t Break the Trial
In another study, a participant missed a scheduled visit due to illness, raising concerns about protocol compliance. The team reviewed the protocol, documented the deviation, completed follow-up assessments, and allowed the participant to continue as described in standard clinical study conduct practices outlined by ClinicalTrials.gov.
Conclusion
Clinical trial protocols form the backbone of how clinical research is planned, executed, and evaluated. They bring together scientific intent, participant safety, regulatory expectations, and operational clarity into a single framework that guides decisions throughout the life of a trial.
For anyone building a career in clinical research, protocol knowledge goes beyond understanding procedures; it reflects the ability to think critically, act responsibly, and respond correctly when real-world challenges arise. Strong protocol understanding supports ethical conduct, improves cross-functional collaboration, and ensures consistency across trial sites.
At CliniLaunch Research Institute, we approach protocol knowledge in our clinical research training programs as a critical capability to develop, not just a document to follow. Ultimately, mastering the protocol is what enables clinical research professionals to contribute meaningfully to high-quality, credible research and build sustainable careers in the field. This is why understanding what is clinical trial protocol is foundational for anyone serious about a career in clinical research.
Frequently Asked Questions (FAQs)
1. What is a clinical trial protocol in simple terms?
A clinical trial protocol is a detailed plan that explains how a clinical study will be conducted, including who can participate, what treatment is given, how safety is monitored, and how results are analyzed.
2. Why is a clinical trial protocol required before starting a study?
A protocol is required to ensure the trial is scientifically sound, ethically conducted, and safe for participants. It prevents decisions from being made midway and ensures consistency across all study sites.
3. Who prepares the clinical trial protocol?
Clinical trial protocols are developed collaboratively by sponsors, investigators, statisticians, and regulatory experts to ensure scientific validity, feasibility, and regulatory compliance.
4. Can a clinical trial protocol be changed after the study starts?
Yes. A protocol can be modified through approved protocol amendments if new safety, scientific, or operational information arises. Any change must be reviewed and approved before implementation.
5. What happens if a protocol is not followed?
When a protocol is not followed, it is documented as a protocol deviation. Deviations are reviewed to assess their impact on participant safety and data quality and do not automatically invalidate a study.
6. How is a clinical trial protocol different from informed consent?
The protocol is a technical document used by the research team, while the informed consent form is written for participants to help them understand the study and voluntarily agree to participate.
7. Why is protocol knowledge important for clinical research careers?
Protocol knowledge helps professionals make correct decisions, handle real-world trial situations, and communicate effectively across teams. It is a core skill evaluated in clinical research roles.
8. Do beginners need to understand statistics in a clinical trial protocol?
Yes, at a basic level. Understanding concepts like sample size, endpoints, and statistical power helps professionals understand why trials are designed in a certain way and how results are interpreted.
9. Are clinical trial protocols the same across all studies?
No. While protocols follow standard guidelines such as ICH Good Clinical Practice, each protocol is customized based on the study objective, population, and treatment being evaluated.
Site monitoring in clinical trials is the process of overseeing study conduct at investigator sites to ensure protocol compliance, patient safety, data accuracy, and regulatory compliance. It is primarily carried out by Clinical Research Associates through planned monitoring visits across the trial lifecycle.
Site monitoring in clinical trials is a critical control mechanism that ensures a study is conducted exactly as approved. It exists to confirm that clinical trial activities follow the protocol, meet regulatory compliance requirements, and uphold ethical standards throughout the trial lifecycle.
At the center of this process is the Clinical Research Associate (CRA), who serves as the operational link between the sponsor and the investigator site. Through structured site monitoring visits, the CRA verifies that patient safety is protected, trial data is accurate and traceable, and essential documents are properly maintained.
Errors in trial conduct or documentation, if left undetected, can compromise data integrity, delay regulatory submissions, or raise serious compliance concerns during inspections. For this reason, site monitoring in clinical trials is not a routine formality. It is a safeguard that supports clinical trial oversight and ensures that studies generate reliable and credible results.
This blog explains what site monitoring in clinical trials involves, the different types of clinical trial monitoring used in practice, and the step-by-step site monitoring process followed from site setup to study close-out, supported by a real-world case example.
What is Clinical Trial Monitoring?
Clinical trial monitoring is a systematic process used to ensure that a clinical study is conducted, recorded, and reported in accordance with the approved protocol, Good Clinical Practice (GCP), regulatory requirements, and ethical principles.
In practical terms, clinical trial monitoring functions as an ongoing quality control activity. It focuses on verifying that participant rights and safety are protected, that adverse event reporting is accurate and timely, and that trial data reflects what actually occurred at the site. This includes reviewing source documents, confirming protocol compliance, and ensuring that deviations are identified, documented, and addressed appropriately.
An important aspect of site monitoring in clinical trials is its role in maintaining regulatory inspection readiness. Well-monitored sites are more likely to demonstrate compliance because essential documents, such as the Investigator Site File and Trial Master File, are kept current and complete. Through regular monitoring, sponsors gain confidence that the trial is being conducted as intended and that the data generated can withstand regulatory review.
Types of Clinical Trial Monitoring
Clinical trials differ in complexity, risk profile, geographic spread, and data volume. For this reason, site monitoring in clinical trials is not performed using a single fixed approach. Instead, different types of clinical trial monitoring are applied based on study needs, regulatory expectations, and risk assessment outcomes.
Each monitoring method serves a specific purpose, and in practice, most trials use a combination rather than relying on only one approach.
On-Site Monitoring
On-site monitoring is the traditional and most direct form of site monitoring in clinical trials. In this approach, the Clinical Research Associate conducts monitoring visits by physically visiting the investigator site. These visits allow the CRA to directly observe trial conduct and verify that study procedures are being followed exactly as described in the protocol.
During an on-site monitoring visit, the CRA reviews source documents to perform source data verification, checks informed consent documentation, assesses adverse event reporting, and evaluates drug accountability and storage conditions. Essential documents maintained in the Investigator Site File are also reviewed to confirm regulatory compliance.
Because the CRA is present at the site, on-site monitoring allows for immediate clarification of issues and direct interaction with site staff. However, it is time-intensive and contributes significantly to monitoring-related costs in clinical trials.
Remote Site Monitoring
Remote site monitoring allows the CRA to conduct monitoring activities without physically visiting the site. Instead, monitoring is performed using secure electronic systems such as Electronic Data Capture platforms, electronic Trial Master Files, and Clinical Trial Management Systems.
Through remote monitoring, the CRA can review trial data, track protocol deviations, assess documentation completeness, and follow up on monitoring findings in a timely manner. This approach improves efficiency, reduces travel requirements, and allows more frequent data review compared to traditional on-site visits.
Remote site monitoring is particularly effective for ongoing data checks and document reviews. However, it has limitations when it comes to verifying physical processes, investigational product handling, and site facilities.
Centralized Monitoring
Centralized monitoring is a data-focused approach in which study data from all participating sites is reviewed centrally by the sponsor or contract research organization. Using statistical tools and data analytics, centralized monitoring helps identify trends, outliers, missing data, or unusual patterns that may indicate quality or compliance issues.
This method supports early risk detection across multiple sites and enhances overall clinical trial oversight. Centralized monitoring is especially useful in large, multi-center studies where consistent site-level issues may not be immediately visible through individual monitoring visits.
While centralized monitoring strengthens trial-level oversight, it does not replace site-level verification and is typically used alongside on-site or remote monitoring.
Risk-Based Monitoring (RBM)
Risk-based monitoring is an approach that focuses monitoring efforts on the aspects of a trial that pose the greatest risk to participant safety and data integrity. Instead of applying the same level of monitoring to all sites and activities, RBM uses predefined risk assessments and ongoing data evaluation to guide monitoring intensity.
Under risk-based monitoring, high-risk processes such as informed consent, primary endpoint data, and safety reporting receive greater attention, while lower-risk activities may be monitored less frequently. This approach allows resources to be used more effectively while maintaining regulatory compliance.
RBM typically combines centralized monitoring, remote monitoring, and targeted on-site monitoring as part of a structured site monitoring plan.
Hybrid Monitoring
Hybrid monitoring combines elements of on-site and remote monitoring. In this approach, critical activities such as source data verification, informed consent verification, and drug accountability are performed during on-site visits, while routine data reviews and document checks are handled remotely.
Hybrid monitoring provides a balanced approach, maintaining oversight of high-risk areas while improving efficiency. As clinical trials increasingly adopt digital systems, hybrid monitoring has become a widely used model in modern studies.
Comparison on types of clinical trial monitoring
Monitoring Type
Where It Happens
Key Activities
Strengths
Limitations
On-Site Monitoring
At the clinical trial site
SDV, IP checks, IC review, facility observation
Most comprehensive; direct oversight
Time-consuming; travel cost
Remote Monitoring
Off-site (online review)
EDC review, document checks, communication
Fast, cost-effective, continuous access
Limited ability to verify physical processes
Centralized Monitoring
Sponsor/CRO central systems
Data analytics, trend checks, anomaly detection
Early detection of deviations across sites
Does not replace site-level verification
Risk-Based Monitoring (RBM)
Combination of methods
Risk assessment, targeted checks
Optimizes resources; focuses on critical risks
Requires strong data systems & planning
Hybrid Monitoring
Mix of on-site + remote
Critical tasks on-site, routine tasks remote
Balanced efficiency and quality
Coordination needed between monitoring types
Clinical Trial Monitoring Step-by-Step Process
The site monitoring process in clinical trials follows a structured sequence of visits conducted across the study lifecycle. Each stage serves a distinct purpose, but together they ensure protocol compliance, patient safety monitoring, and data integrity from study start to closure.
The Clinical Research Associate is responsible for planning, executing, documenting, and following up on these monitoring activities as part of ongoing clinical trial oversight.
Pre-Study Visit (PSV): Assessing Site Readiness
The Pre-Study Visit is conducted before a site is authorized to participate in a clinical trial. Its primary objective is to assess whether the site is capable of conducting the study in accordance with the protocol and regulatory requirements.
During the PSV, the CRA evaluates the site’s infrastructure, including clinical facilities, investigational product storage areas, and data handling systems. The qualifications and experience of the investigator and site staff are reviewed to ensure they are appropriate for the study. The CRA also assesses whether the site can manage essential documents, adverse event reporting, and patient records in a compliant manner.
This visit plays a preventive role. By identifying gaps early, the CRA can guide the site on corrective actions before trial initiation, reducing the risk of compliance issues later in the study.
Site Initiation Visit (SIV): Preparing the Site for Trial Conduct
The Site Initiation Visit formally marks the transition from site preparation to active trial conduct. At this stage, the CRA ensures that the site fully understands the study requirements and is ready to enroll participants.
During the SIV, the CRA reviews the approved protocol in detail with the site team, explaining study objectives, eligibility criteria, visit schedules, and safety reporting expectations. Training is provided on informed consent procedures, data entry into the EDC system, and handling of investigational products. The CRA also confirms that all essential documents are in place and that the site monitoring plan is clearly understood.
A well-executed SIV establishes consistency in trial conduct and reduces the likelihood of protocol deviations during enrollment and follow-up.
Routine monitoring visits are conducted at regular intervals throughout the trial and represent the core of site monitoring in clinical trials. These visits allow the CRA to verify that the study continues to be conducted as approved.
During routine monitoring visits, the CRA reviews participant eligibility, confirms that informed consent was obtained correctly, and monitors patient safety through adverse event reporting. Data entered into the CRF or EDC system is compared with source documents as part of source data verification. The CRA also reviews the Investigator Site File to ensure that essential documents remain current and complete.
Any issues identified during these visits are documented as monitoring findings. The CRA works with the site to resolve these issues and, where necessary, supports corrective and preventive actions to prevent recurrence.
Close-Out Visit: Completing Site Responsibilities
The Close-Out Visit is conducted once all trial activities at the site have been completed. The purpose of this visit is to ensure that the site has fulfilled all protocol, regulatory, and documentation requirements before the study is formally closed.
During the close-out visit, the CRA confirms that all data queries have been resolved and that the study data is complete and accurate. Essential documents are reviewed to ensure proper archiving, and regulatory compliance is verified. The CRA also ensures that investigational products are returned or destroyed according to the protocol and applicable regulations.
This final monitoring stage ensures that the site is prepared for audits or inspections and that the study can progress confidently toward analysis and reporting.
Case Study on Clinical Trial Monitoring
How a Routine Monitoring Visit Prevented Data Integrity Issues
This case illustrates how effective site monitoring in clinical trials directly protects data quality and scientific validity.
During a routine monitoring visit, the Clinical Research Associate observed that a study participant scheduled for a Day 5 visit arrived nearly two hours later than planned. Despite the delay, the site staff proceeded with dosing and pharmacokinetic (PK) or pharmacodynamic (PD) sample collection without documenting the deviation or questioning its impact.
At first glance, the situation appeared operationally minor. However, in clinical trials involving PK or PD assessments, sample timing is critical. Even small deviations can significantly affect data interpretation.
Identification of the Issue
When the CRA later reviewed the source documents, a serious discrepancy became evident. The visit was documented as if it had occurred exactly according to the protocol-defined schedule. There was no record of the delayed arrival, no protocol deviation reported, and the PK or PD sample times were recorded based on planned rather than actual collection times.
This meant that the recorded data did not accurately reflect what occurred at the site. Because PK analyses depend on precise timing relative to dosing, the inaccurate documentation had the potential to distort the participant’s concentration profile and compromise the scientific integrity of the dataset.
CRA Action and Follow-Up
Having directly observed the deviation, the CRA escalated the issue to the Principal Investigator and the sponsor. The CRA ensured that the source documents were corrected to reflect the actual visit and sample collection times and that a formal protocol deviation was documented.
In addition, the CRA supported corrective and preventive actions. These included targeted protocol and GCP retraining for the site staff and the introduction of a checklist to reinforce real-time documentation during critical visits. These actions were aimed at preventing similar issues in future visits.
Outcome and Key Learning
Because the issue was identified and addressed promptly, inaccurate PK data was prevented from entering the final analysis. The CRA’s intervention preserved the reliability of the study data and supported regulatory compliance.
This case highlights the value of routine monitoring visits and demonstrates how vigilant site monitoring helps protect patient safety, data integrity, and overall trial credibility. It also reinforces why site monitoring is a critical safeguard rather than a procedural formality.
Conclusion
Site monitoring is one of the most operationally critical functions in clinical trials. It is where protocol design, regulatory expectations, and real-world site execution intersect. Understanding how site monitoring works—across different monitoring types and visit stages—provides a practical view of how clinical trials are actually controlled and safeguarded.
For individuals looking to enter clinical research, this knowledge is not optional. Roles such as Clinical Research Coordinator, Clinical Trial Assistant, and Clinical Research Associate all require a working understanding of site monitoring, protocol compliance, essential documentation, and patient safety oversight.
At CliniLaunch Research Institute, the PG Diploma in Clinical Research is designed to build this exact operational understanding. The program focuses on real clinical trial workflows, including site monitoring processes, CRA responsibilities, regulatory compliance, and inspection readiness—preparing learners to function confidently in entry-level and growing clinical research roles.
For those aiming to move from academic knowledge to industry-ready capability, structured training aligned with real trial operations makes the difference.
Frequently Asked Questions (FAQs)
Who decides how site monitoring will be conducted in a clinical trial?
The sponsor, often with input from the CRO, defines the site monitoring plan. This plan outlines the monitoring approach, visit frequency, and responsibilities based on study risk and complexity.
Is site monitoring mandatory for all clinical trials?
Yes. Some form of site monitoring is required for all interventional clinical trials. The method may vary, but oversight of site activities is always expected by regulators.
Can a clinical trial run without on-site monitoring?
In some studies, monitoring may rely more on remote or centralized methods. However, critical activities such as informed consent and investigational product handling usually still require on-site verification at some stage.
What happens if monitoring issues are not corrected?
Unresolved monitoring findings can lead to protocol deviations, regulatory observations, delayed approvals, or rejection of trial data during inspections.
How are monitoring findings documented?
Monitoring findings are recorded in a monitoring visit report. The site is required to respond, and corrective and preventive actions are tracked until closure.
Does site monitoring replace audits or inspections?
No. Site monitoring is a routine oversight activity. Audits and regulatory inspections are independent reviews conducted by sponsors or authorities to assess overall compliance.
Is site monitoring only the responsibility of the CRA?
The CRA leads monitoring activities, but investigators and site staff are responsible for correcting issues and maintaining compliance at the site.
Why do beginners struggle with site monitoring concepts?
Most academic programs focus on theory, while site monitoring involves operational decision-making, documentation control, and real-time risk management that are learned through practice.
This Blog explores practical biomedical engineering career alternatives that align with how the healthcare and life sciences industry operates today. For many biomedical engineers, career realities differ from expectations set during their academic years. While the degree prepares graduates for innovation. While the degree builds strong foundations in innovation and medical technology, the availability of core roles remains limited across regions. This gap has led many graduates to actively explore alternative careers for biomedical engineers that better align with current industry demand.
Even professionals working in core biomedical roles often experience slow growth, limited specialization, and reduced exposure to high-value areas. At the same time, the healthcare ecosystem is evolving rapidly, driven by digital platforms, data-intensive clinical systems, AI-enabled diagnostics, cloud infrastructure, and stricter regulations. As a result, choosing an alternative career for biomedical engineers has become a practical and sometimes necessary step to remain relevant and future ready.
A 2021 BME Career Exploration study highlights this shift, showing that many graduates now transition into regulated, data-driven, and technology-enabled healthcare roles. These alternative career paths for biomedical engineers leverage core strengths such as systems thinking, analytical ability, and biological understanding, offering clearer growth pathways and long-term career stability. As a result, many graduates now actively consider non-core jobs for biomedical engineers that offer clearer growth, stability, and industry alignment.
The sections below outline how each alternative career for biomedical engineers aligns with current healthcare industry needs, skill requirements, and long-term growth potential. Understanding how different roles evolve over time helps biomedical graduates evaluate long-term biomedical engineers’ career paths beyond traditional assumptions.
Alternative careers for biomedical engineers
The following sections outline structured healthcare careers for biomedical engineers that leverage medical knowledge, regulatory awareness, and system-based thinking.
1. Clinical Research roles
Below are some of the most practical and industry-relevant who want to work beyond traditional core engineering roles while staying connected to healthcare.
Entry-Level Roles You Can Target
Clinical Data Coordinator
Clinical Data Associate
Clinical Trial Assistant (CTA)
Clinical Research Coordinator (CRC)
Pharmacovigilance Associate / Drug Safety Associate
These clinical research roles for biomedical engineers focus on trial execution, data integrity, and regulatory compliance across global studies.
Clinical research focuses on executing and managing clinical trials that test the safety and effectiveness of drugs, devices, and therapies. The work is centered around patient data, documentation, timelines, and regulatory compliance. These roles ensure trials are conducted strictly as per protocol so that results are acceptable to regulators. This is structured, process-driven execution, not discovery research or analytics.
Why Biomedical Engineers Fit Well
Biomedical engineers fit well into clinical research because they are comfortable with structured data, medical terminology, and regulated workflows. The roles reward consistency, attention to detail, and protocol adherence rather than innovation or design. For BMEs who want to stay close to healthcare systems and real-world clinical impact, this is a practical and stable career path.
Career Progression, Salary, and Companies
Career progression (typical): Entry-level role → Senior Associate / Analyst → Manager (role-specific) Growth depends on trial exposure, process mastery, and regulatory experience.
Average entry-level salary (India): Most entry-level clinical research roles start between ₹2.5–4.5 LPA, depending on role, organization, and city. CROs generally offer more consistent compensation than hospital-based roles.
Hospitals and academic research centers conducting sponsored trials
Outlook: Clinical research remains stable as regulatory trials continue irrespective of market cycles. With trials becoming more global and data-intensive, the demand for compliant, well-documented execution continues to rise.
How to Get Started
Start by identifying one entry-level role and aligning your preparation toward it rather than applying broadly. Build a clear understanding of the clinical trial lifecycle, GCP principles, and role-specific workflows. For candidates without industry exposure, a structured program like Advance Diploma in Clinical Research helps bridge the gap by providing domain context, practical workflows, and hiring alignment. If internships or site-level opportunities are accessible, they should be pursued alongside or immediately after training. Networking with professionals already working in CROs or trial sites helps clarify expectations early and avoid misaligned roles.
Aspect
Details
Domain
Clinical Research
Core Focus
Trial execution, data integrity, documentation, compliance
Entry-Level Roles
CDM, CTA, CRC, PV, Regulatory, Clinical Ops, Medical Writing
Entry Salary (India)
₹2.5–4.5 LPA (average)
Hiring Organizations
CROs, Pharma, Biotech, Hospitals
Key Skills Needed
GCP basics, process discipline, clinical context
Career Growth
Associate → Analyst → Manager
Long-Term Outlook
Stable, compliance-driven, globally relevant
Advanced Diploma in
Clinical Research
Develop industry-ready clinical research skills used across pharmaceutical companies, CROs, and healthcare organizations. Learn how clinical trials are designed, conducted, monitored, and regulated, while gaining hands-on exposure to real-world clinical research workflows and compliance standards.
Clinical Trial Management, ICH-GCP & Regulatory Compliance, Clinical Data Management Basics, Pharmacovigilance Fundamentals, Trial Documentation & Monitoring, Ethics Committees & Audits, Career Role Readiness (CRA, CTA, CDM)
Other Courses
Clinical SAS
Medical Coding
Biostatistics
2.Medical Coding roles
Entry-Level Roles You Can Target
Medical Coder (ICD-10 / CPT – Trainee / Junior)
Certified Professional Coder (CPC – Entry Level)
Medical Coding Analyst (Junior)
Healthcare Documentation Specialist
Medical Billing & Coding Associate
Revenue Cycle Management (RCM) Associate
Medical coding jobs for biomedical engineers offer a structured, documentation-driven path within healthcare operations. Documentation-driven and compliance-focused roles represent some of the most accessible biomedical engineering jobs outside core engineering functions.
Medical coding focuses on translating clinical documentation such as physician notes, discharge summaries, diagnostic reports, and procedure records into standardized medical codes used for billing, reimbursement, audits, and compliance. The work is documentation-heavy, rule-based, and governed by strict coding guidelines and payer regulations. Accuracy and consistency are critical, as coding errors directly affect revenue, audits, and legal compliance. This is operational healthcare work, not clinical decision-making or biomedical research.
Why Biomedical Engineers Fit Well
Biomedical engineers fit well into medical coding because they already understand medical terminology, human anatomy, disease processes, and clinical workflows. The role rewards attention to detail, structured interpretation of medical records, and adherence to classification standards rather than engineering design or innovation. For BMEs who prefer stable, desk-based healthcare roles with clear rules and measurable output, medical coding offers a predictable and scalable career path.
Career Progression, Salary, and Companies
Career progression (typical): Junior Medical Coder → Senior Coder / Coding Analyst → Auditor / Team Lead → Coding Manager / Compliance Specialist.
Growth depends on coding accuracy, certification upgrades, specialty exposure (e.g., inpatient, surgical, risk adjustment), and audit experience.
Average entry-level salary (India): Most entry-level medical coding roles start between ₹2.0–4.0 LPA, depending on certification status, organization, and city. Certified coders generally progress faster than non-certified entrants.
Outlook: Medical coding remains stable due to the ongoing need for standardized billing, insurance processing, and regulatory audits. While automation assists in coding, human coders are still required for complex cases, audits, and compliance-driven reviews, ensuring steady demand.
How to Get Started
Start by deciding whether you want to pursue outpatient, inpatient, or specialty coding instead of treating medical coding as a single generic role. Build strong fundamentals in ICD-10-CM, CPT, and medical documentation standards, as accuracy and guideline interpretation matter more than speed at the entry level. For candidates without prior healthcare operations exposure, a structured program such as a Advanced Diploma in Medical Coding help bridge the gap by providing coding framework clarity, real-world chart interpretation practice, and alignment with hiring expectations. Entry-level production roles or internships are critical to gaining volume-based experience and improving productivity benchmarks. Networking with experienced coders and auditors helps candidates understand certification value, audit expectations, and long-term growth paths early.
Build industry-ready skills in medical coding used across hospitals, healthcare providers, insurance companies, and global healthcare services. Learn to accurately convert medical diagnoses, procedures, and services into standardized codes while ensuring compliance, accuracy, and reimbursement of integrity.
Pharmacovigilance Associate / Drug Safety Associate
Case Processing Associate
Safety Data Associate
Argus Safety / PV Systems Associate (Junior)
Pharmacovigilance Executive
Clinical Safety Coordinator
Pharmacovigilance careers for biomedical engineer’s center on safety monitoring, adverse event reporting, and regulatory compliance.
Pharmacovigilance focuses on monitoring, evaluating, and reporting the safety of drugs, vaccines, and medical products during clinical development and post-marketing use. The work involves adverse event processing, safety data review, and regulatory reporting to global health authorities. These roles ensure that safety risks are identified, documented, and communicated accurately across the product lifecycle. This is compliance-driven safety surveillance, not laboratory research or clinical decision-making.
Why Biomedical Engineers Fit Well
Biomedical engineers fit well into pharmacovigilance because they are familiar with medical terminology, disease mechanisms, and structured documentation. The role requires careful interpretation of clinical narratives, attention to detail, and adherence to regulatory standards rather than engineering design or experimentation. For BMEs who prefer analytical, documentation-focused healthcare roles with regulatory relevance, drug safety offers a stable and well-defined career path.
Career Progression, Salary, and Companies
Career progression (typical): Drug Safety Associate → Senior Safety Associate → Safety Scientist / PV Lead → Safety Manager
Growth depends on case complexity exposure, regulatory knowledge, safety database experience, and therapeutic area specialization.
Average entry-level salary (India): Most entry-level pharmacovigilance roles start between ₹2.5–5.0 LPA, depending on organization, role scope, and city.
Companies you can apply to:
CROs: IQVIA, ICON, Parexel
Pharma / Biotech companies with in-house safety teams
Pharmacovigilance service providers
Outlook: Pharmacovigilance remains stable due to increasing regulatory scrutiny and global safety reporting requirements. Demand continues if drugs and vaccines remain in use worldwide.
How to Get Started
Begin by understanding core pharmacovigilance workflows such as adverse event reporting, case processing, MedDRA coding, and global regulatory requirements. Candidates should align their preparation toward specific entry-level roles rather than applying broadly. For those without prior industry exposure, a structured program like the Advanced Diploma in Clinical Research, where pharmacovigilance and drug safety are covered as a dedicated module, helps bridge the gap by providing regulatory context and practical workflow understanding. Entry-level roles in CROs or safety teams provide the exposure needed to build accuracy and long-term role clarity.
Aspect
Details
Domain
Pharmacovigilance & Drug Safety
Core Focus
Safety monitoring, case processing, regulatory reporting
Entry-Level Roles
Drug Safety Associate, PV Executive, Case Processor
Entry Salary (India)
₹2.5–5.0 LPA (average)
Hiring Organizations
CROs, Pharmaceutical companies, PV service providers
Regulatory affairs jobs after biomedical engineering focus on compliance, submissions, and interaction with health authorities.
Regulatory affairs focus on ensuring that drugs, medical devices, and clinical studies comply with national and international regulatory requirements. The work involves preparing, reviewing, and maintaining regulatory documents, coordinating submissions, tracking approvals, and supporting interactions with health authorities. These roles ensure products and trials meet defined regulatory standards before and after approval. This is documentation- and compliance-driven work, not laboratory research or product development.
Why Biomedical Engineers Fit Well
Biomedical engineers fit well into regulatory affairs because they understand medical concepts, product lifecycles, and structured documentation requirements. The role rewards attention to detail, interpretation of guidelines, and consistency in regulatory communication rather than innovation or experimentation. For BMEs who prefer policy-aligned, process-oriented roles that influence product approvals and compliance, regulatory affairs offer a clear and stable career path.
Outlook: Regulatory affairs remain stable as approval requirements continue to expand globally. Increasing regulatory complexity across regions sustains demand for trained regulatory professionals.
How to Get Started
Start by understanding regulatory fundamentals such as submission types, approval pathways, and global guidelines governing drugs and medical devices. Candidates should prepare specific entry-level roles rather than applying broadly across regulatory functions. For those without industry exposure, a structured program like the Advanced Diploma in Clinical Research, which includes regulatory affairs as a core module, helps build regulatory context, documentation familiarity, and workflow understanding. Entry-level roles in pharma companies or CRO regulatory teams provide practical exposure to submissions and compliance processes. Early networking with regulatory professionals helps clarify specialization paths and expectations.
Biomedical engineers fit well into quality assurance because they are trained to work with structured processes, technical documentation, and regulated environments. The role values attention to detail, risk awareness, and consistency in following procedures rather than innovation or design work. For BMEs who prefer governance-oriented roles that influence compliance and operational quality across healthcare systems, QA offers a stable and well-defined career option.
Career Progression, Salary, and Companies
Career progression (typical): QA Associate → Senior QA Associate → QA Manager → Quality Lead / Head
Growth depends on audit exposure, regulatory knowledge, SOP management experience, and cross-functional coordination.
Average entry-level salary (India): Most entry-level quality assurance roles start between ₹3.0–5.0 LPA, depending on organization, domain, and city.
Companies you can apply to:
CROs: IQVIA, Parexel
Pharma & Biotech companies
Medical device manufacturers
Hospitals and research organizations with QA teams
Outlook: Quality assurance remains stable as regulatory inspections; audits, and compliance requirements continue to intensify globally. Demand persists across clinical research, pharma, and healthcare operations.
How to Get Started
Begin by understanding quality fundamentals such as SOPs, GxP guidelines, deviation management, and audit processes. Candidates should align their preparation toward entry-level QA roles rather than applying broadly across departments. For those without industry exposure, a structured program like the Advanced Diploma in Clinical Research, which includes quality assurance as a core module, helps build compliance context, documentation familiarity, and workflow understanding. Entry-level roles in CROs or regulated organizations provide practical exposure to audits and quality systems. Early interaction with QA professionals helps clarify long-term specialization paths.
Aspect
Details
Domain
Quality Assurance
Core Focus
Compliance, audits, SOP adherence
Entry-Level Roles
QA Associate, Compliance Executive
Entry Salary (India)
₹3.0–5.0 LPA (average)
Hiring Organizations
CROs, Pharma, Medical Devices, Hospitals
Key Skills Needed
Documentation, process discipline, GxP basics
Career Growth
Associate → Manager → Lead
Long-Term Outlook
Stable, audit-driven, globally relevant
6.Health Informatics roles
Entry-Level Roles You Can Target
Health Informatics Associate
Clinical Informatics Coordinator
Healthcare Data Analyst (Junior)
EHR / EMR Support Analyst
Health Information Management (HIM) Executive
Clinical Systems Support Associate
A health informatics career path combines healthcare data, clinical systems, and technology-enabled workflows.
Health informatics focuses on managing, analyzing, and optimizing healthcare data generated from clinical systems such as electronic health records, hospital information systems, and clinical databases. The work involves data accuracy, system workflows, interoperability, reporting, and supporting clinicians and administrators in using health data effectively. These roles sit at the intersection of healthcare, IT systems, and data governance. This is systems and data coordination work, not clinical practice or biomedical research.
Why Biomedical Engineers Fit Well
Biomedical engineers fit well into health informatics because they understand clinical workflows, medical terminology, and system-based thinking. The role requires interpreting healthcare data, working with structured systems, and supporting technology-driven care delivery rather than engineering design or experimentation. For BMEs who want to work with healthcare data and digital systems while staying close to clinical environments, health informatics offers a practical and evolving career path.
Career Progression, Salary, and Companies
Career progression (typical): Health Informatics Associate → Informatics Analyst → Senior Analyst / Consultant → Informatics Manager
Growth depends on system exposure, healthcare domain knowledge, data handling skills, and familiarity with clinical information systems.
Average entry-level salary (India): Most entry-level health informatics roles start between ₹3.0–5.5 LPA, depending on organization, system complexity, and city.
Companies you can apply to:
Hospitals and healthcare networks using digital health systems
CROs and pharma organizations with informatics teams
Outlook: Health informatics continues to grow as healthcare systems digitize, and data-driven care becomes standard. Demand increases with expanding EHR adoption, interoperability requirements, and healthcare analytics needs.
How to Get Started
Begin by understanding healthcare data flows, EHR concepts, clinical documentation standards, and basic health data governance. Candidates should target specific entry-level informatics or clinical systems roles rather than applying broadly across IT or analytics positions. At CliniLaunch Research Institute, relevant programs such as the PG Diploma in AI/ML in Healthcare and clinical research programs that expose learners to healthcare data systems and clinical workflows help build foundational informatics understanding. Entry-level roles in hospitals, health IT teams, or healthcare analytics firms provide practical exposure to real-world systems and data environments.
Aspect
Details
Domain
Health Informatics
Core Focus
Healthcare data systems, EHRs, clinical workflows
Entry-Level Roles
Informatics Associate, EHR Analyst
Entry Salary (India)
₹3.0–5.5 LPA (average)
Hiring Organizations
Hospitals, Health IT firms, Analytics companies
Key Skills Needed
Clinical data understanding, systems thinking
Career Growth
Associate → Analyst → Manager
Long-Term Outlook
Growing, data-driven, healthcare-focused
7. Digital Health roles
Entry-Level Roles You Can Target
Digital Health Executive
Health Technology Associate
Clinical Digital Operations Associate
Digital Health Project Coordinator
Healthcare Technology Support Analyst
Digital Health Data Associate (Junior)
Digital health jobs for biomedical engineers involve supporting technology platforms used in modern healthcare delivery.
Digital health focuses on the use of technology to improve healthcare delivery, patient monitoring, clinical workflows, and health data management. The work involves supporting digital platforms such as telemedicine systems, remote patient monitoring tools, clinical dashboards, and healthcare applications. These roles bridge healthcare operations and technology by ensuring digital tools are implemented, used, and maintained effectively. This is technology-enabled healthcare operations, not software development or clinical practice.
Why Biomedical Engineers Fit Well
Biomedical engineers fit well into digital health because they understand both healthcare systems and technology-driven workflows. The role values systems thinking, clinical context awareness, and the ability to work across medical and technical teams rather than pure coding or engineering design. For BMEs who want to be part of healthcare innovation without moving into core IT development roles, digital health offers a flexible and future-facing career path.
Career Progression, Salary, and Companies
Career progression (typical): Digital Health Associate → Digital Health Analyst → Senior Analyst / Consultant → Digital Health Manager
Growth depends on platform exposure, healthcare domain knowledge, data handling skills, and cross-functional coordination.
Average entry-level salary (India): Most entry-level digital health roles start between ₹3.0–6.0 LPA, depending on organization, role scope, and city.
Companies you can apply to:
Digital health and health-tech companies
Hospitals adopting telemedicine and digital care platforms
Healthcare analytics and technology consulting firms
Pharma and CROs implementing digital trial solutions
Outlook: Digital health continues to expand as healthcare systems adopt virtual care, remote monitoring, and data-driven decision-making. Demand is driven by technology adoption rather than traditional healthcare hiring cycles.
How to Get Started
Begin by understanding digital health fundamentals such as telemedicine workflows, healthcare data integration, digital clinical platforms, and patient engagement systems. Candidates should target entry-level digital health or healthcare technology coordination roles rather than generic IT positions. At CliniLaunch Research Institute, programs such as the PG Diploma in AI/ML in Healthcare and clinical research programs provide exposure to healthcare data, digital tools, and clinical workflows that are directly relevant to digital health roles. This combination helps learners understand how technology, data, and clinical operations intersect in real healthcare environments. Entry-level roles in health-tech companies or hospital digital teams provide practical exposure to digital healthcare systems.
Aspect
Details
Domain
Digital Health
Core Focus
Healthcare technology, digital platforms, workflows
Healthcare context, systems thinking, coordination
Career Growth
Associate → Analyst → Manager
Long-Term Outlook
Growing, technology-driven, healthcare-focused
8. Data Analytics roles
Data Analytics roles
Data Analyst (Junior)
Healthcare Data Analyst
Clinical Data Analyst (Non-statistical)
Business / Reporting Analyst (Healthcare)
Data Operations Associate
Analytics Support Associate
Healthcare data analytics careers focus on turning clinical and operational data into actionable insights.
Data analytics focuses on collecting, cleaning, analyzing, and interpreting structured data to support decision-making. In healthcare and life sciences, this includes clinical data, operational metrics, patient outcomes, and business performance data. The work involves dashboards, reports, trend analysis, and data validation rather than predictive modeling or advanced research. These roles support operational and strategic decisions using existing data systems. This is applied data analysis, not core data science or algorithm development.
Why Biomedical Engineers Fit Well
Biomedical engineers fit well into data analytics because they are comfortable working with data, structured problem-solving, and interpreting technical information within a healthcare context. The role values analytical thinking, logical reasoning, and the ability to translate data into meaningful insights rather than deep programming or mathematical research. For BMEs who want to work with data while staying connected to healthcare and life sciences, data analytics offers a flexible and transferable career option.
Career Progression, Salary, and Companies
Career progression (typical): Junior Data Analyst → Data Analyst → Senior Analyst → Analytics Manager / Lead
Growth depends on domain expertise, data handling skills, reporting accuracy, and exposure to real business or clinical datasets.
Average entry-level salary (India):
Most entry-level data analytics roles start between ₹3.0–6.0 LPA, depending on industry, tools used, and organization.
Companies you can apply to:
Healthcare and life sciences organizations
Analytics and consulting firms
Hospitals and health-tech companies
CROs and pharma companies using data-driven operations
Outlook: Data analytics remain in demand as organizations rely increasingly on data for operational efficiency and decision-making. In healthcare, demand continues due to growing data volumes and digital system adoption.
How to Get Started
Begin by understanding data analytics fundamentals such as data cleaning, basic statistics, reporting, and visualization. Candidates should focus on entry-level analyst roles rather than advanced data science positions. At CliniLaunch Research Institute, programs like the PG Diploma in AI/ML in Healthcare provide exposure to healthcare datasets, analytical tools, and applied use cases that are relevant to analytics roles. This foundation helps learners connect data analysis with real healthcare and clinical scenarios. Entry-level analysts or reporting roles provide the practical experience needed to grow within the analytics domain.
How to Get Started
Begin by understanding data analytics fundamentals such as data cleaning, basic statistics, reporting, and visualization. Candidates should focus on entry-level analyst roles rather than advanced data science positions. At CliniLaunch Research Institute, programs like the PG Diploma in AI/ML in Healthcare provide exposure to healthcare datasets, analytical tools, and applied use cases that are relevant to analytics roles. This foundation helps learners connect data analysis with real healthcare and clinical scenarios. Entry-level analysts or reporting roles provide the practical experience needed to grow within the analytics domain.
Aspect
Details
Domain
Data Analytics
Core Focus
Data analysis, reporting, decision support
Entry-Level Roles
Data Analyst, Reporting Analyst
Entry Salary (India)
₹3.0–6.0 LPA (average)
Hiring Organizations
Healthcare firms, Analytics companies
Key Skills Needed
Data handling, analytical thinking, tools
Career Growth
Analyst → Senior Analyst → Manager
Long-Term Outlook
Stable, data-driven, cross-industry
9. Data Science roles
Entry-Level Roles You Can Target
Data Scientist (Junior)
Associate Data Scientist
Machine Learning Analyst (Entry-Level)
Healthcare Data Scientist (Junior)
AI/ML Analyst (Trainee)
Applied Analytics Associate
Data science represents one of the most advanced life sciences career options for biomedical engineers with analytical strengths.
Data science focuses on using data to build predictive models, identify patterns, and support complex decision-making. In healthcare and life sciences, this includes working with clinical data, patient outcomes, operational datasets, and real-world evidence to generate insights using statistical methods and machine learning techniques. The work involves data preparation, model development, validation, and interpretation rather than routine reporting. This is applied to modeling and analytics, not pure software engineering or academic research.
Why Biomedical Engineers Fit Well
Biomedical engineers fit well into data science because they combine analytical thinking with a strong domain understanding of healthcare and biological systems. The role benefits from problem-solving ability, comfort with data-driven reasoning, and the capacity to interpret results within a medical or clinical context. While additional skills in programming and statistics are required, BMEs often adapt well because they already understand the complexity and variability of healthcare data. For those willing to build deeper analytical expertise, data science offers high-impact roles across healthcare and life sciences.
Career Progression, Salary, and Companies
Career progression (typical): Junior Data Scientist → Data Scientist → Senior Data Scientist → Data Science Lead / Manager
Growth depends on model-building capability, domain expertise, problem complexity handled, and business or clinical impact of solutions.
Average entry-level salary (India): Most entry-level data science roles start between ₹4.5–8.0 LPA, depending on skill depth, industry, and organization.
Companies you can apply to:
Healthcare and life sciences analytics firms
Health-tech and AI-driven healthcare companies
Pharma, biotech, and CROs using advanced analytics
Consulting and data science service organizations
Outlook: Data science continues to grow as healthcare organizations adopt AI-driven decision-making and predictive analytics. Demand remains strong for professionals who can combine technical modeling skills with healthcare domain understanding.
How to Get Started
Begin by building strong fundamentals in data handling, statistics, and programming before moving into machine learning concepts. Candidates should target junior or associate data science roles rather than expecting direct entry into advanced modeling positions. At CliniLaunch Research Institute, the PG Diploma in AI/ML in Healthcare provides exposure to healthcare datasets, applied machine learning workflows, and real-world use cases relevant to data science roles. This foundation helps learners connect algorithms with clinical and healthcare problems. Entry-level analytics or ML trainee roles provide the practical experience needed to progress within the data science domain.
Aspect
Details
Domain
Data Analytics
Core Focus
Data analysis, reporting, decision support
Entry-Level Roles
Data Analyst, Reporting Analyst
Entry Salary (India)
₹3.0–6.0 LPA (average)
Hiring Organizations
Healthcare firms, Analytics companies
Key Skills Needed
Data handling, analytical thinking, tools
Career Growth
Analyst → Senior Analyst → Manager
Long-Term Outlook
Stable, data-driven, cross-industry
10. AI & ML in Healthcare
Entry-Level Roles You Can Target
AI/ML Analyst (Healthcare – Junior)
Healthcare Machine Learning Associate
Clinical AI Analyst
Healthcare Data Science Associate (AI-focused)
AI Solutions Analyst (Healthcare)
Applied AI Analyst (Life Sciences)
AI and ML in healthcare careers apply machine learning models to clinical, imaging, and healthcare datasets.
AI and ML in healthcare focus on applying machine learning models and data-driven algorithms to healthcare, clinical, and life sciences data. The work involves developing, testing, and validating models for use cases such as disease prediction, patient risk stratification, medical imaging support, clinical decision support, and operational optimization. These roles sit at the intersection of healthcare data, analytics, and applied machine learning. This is applied to AI work, not software engineering or academic research.
Why Biomedical Engineers Fit Well
Biomedical engineers fit well into AI and ML roles because they understand healthcare data complexity, clinical context, and biological variability. The role requires analytical thinking, problem formulation, and the ability to interpret model outputs in a medical or clinical setting rather than only focusing on algorithms. For BMEs willing to build strong foundations in data handling, statistics, and machine learning, AI and ML in healthcare offer high-impact and future-facing career opportunities.
Career Progression, Salary, and Companies
Career progression (typical): AI/ML Analyst → Machine Learning Engineer / Data Scientist → Senior AI Specialist → AI Lead / Manager.
Growth depends on model deployment exposure, domain-specific use cases handled, and the ability to translate AI outputs into healthcare decisions.
Average entry-level salary (India): Most entry-level AI and ML healthcare roles start between ₹5.0–9.0 LPA, depending on skill depth, tools proficiency, and organization.
Pharma, biotech, and CROs using AI for trials and RWE
Healthcare analytics and AI consulting firms
Hospitals and research organizations adopting AI solutions
Outlook: AI and ML adoption in healthcare continues to expand, driven by increasing data availability and demand for predictive, automated decision-support systems. Roles favor professionals who combine technical skills with healthcare domain understanding.
How to Get Started
Begin by building strong foundations in data analytics, statistics, and programming before moving into machine learning concepts and healthcare use cases. Candidates should target junior or associate AI/ML roles rather than advanced research positions initially. At CliniLaunch Research Institute, the PG Diploma in AI/ML in Healthcare provides structured exposure to healthcare datasets, applied machine learning workflows, and real-world clinical use cases. This helps learners understand how AI models are built, validated, and interpreted within healthcare environments. Entry-level analysts or AI trainee roles provide the practical experience required to progress in this domain.
Aspect
Details
Domain
AI & ML in Healthcare
Core Focus
Applied machine learning, healthcare data modeling
Machine learning fundamentals, data handling, healthcare context
Career Growth
Analyst → Specialist → Lead
Long-Term Outlook
Growing, skill-driven, high-impact
PG Diploma in
AI & ML in Healthcare
Build future-ready skills at the intersection of artificial intelligence and healthcare. Learn how AI and machine learning are applied in clinical research, medical imaging, diagnostics, drug discovery, and healthcare data analytics to solve real-world healthcare problems.
Python for AI & ML, Healthcare Data Analysis, Machine Learning Algorithms, Deep Learning Fundamentals, AI in Medical Imaging & Diagnostics, Predictive Analytics in Healthcare, Real-world Healthcare AI Projects
11. Medical Devices & Application Specialist Roles
Entry-Level Roles You Can Target
Application Specialist (Medical Devices – Junior)
Clinical Application Executive
Product Support Specialist (Medical Devices)
Field Application Associate
Technical Clinical Support Executive
Device Training & Support Associate
Medical device application specialist jobs combine clinical exposure with hands-on device support and training.
Medical device application roles focus on supporting the clinical use, setup, and optimization of medical devices used in hospitals and diagnostic settings. The work involves product demonstrations, user training, troubleshooting, clinical workflow support, and coordination between clinicians and device companies. These roles ensure devices are used safely, effectively, and as intended in real-world healthcare environments. This is application and clinical support work, not device design or core R&D.
Why Biomedical Engineers Fit Well
Biomedical engineers fit well into application specialist roles because they understand medical devices, clinical environments, and technology–user interaction. The role values product knowledge, communication with clinicians, and practical problem-solving rather than engineering design or laboratory research. For BMEs who prefer hands-on clinical exposure and interaction with healthcare professionals, this path offers a direct connection to patient care through technology.
Career Progression, Salary, and Companies
Career progression (typical): Application Specialist → Senior Application Specialist → Product / Clinical Manager → Regional Product Lead
Growth depends on device expertise, clinical exposure, communication skills, and territory or product responsibility.
Average entry-level salary (India): Most entry-level application specialist roles start between ₹3.0–6.0 LPA, depending on device category, organization, and city.
Medical equipment distributors and service partners
Hospitals using advanced medical devices
Outlook: Medical device application roles remain steady as hospitals continue adopting advanced technologies. Demand grows with the introduction of new devices that require structured clinical training and support.
How to Get Started
Begin by understanding basic medical device principles, clinical workflows, and user training requirements. Candidates should target application or clinical support roles rather than pure sales positions. At CliniLaunch Research Institute, exposure gained through the Advanced Diploma in Clinical Research helps learners understand clinical environments, regulatory expectations, and device usage within trials and healthcare settings. Entry-level roles with device companies or distributors to provide hands-on exposure to products and clinical users.
Aspect
Details
Domain
Medical Devices & Applications
Core Focus
Device usage, clinical support, user training
Entry-Level Roles
Application Specialist, Clinical Support
Entry Salary (India)
₹3.0–6.0 LPA (average)
Hiring Organizations
Medical device companies, Hospitals, Distributors
Key Skills Needed
Device knowledge, clinical communication
Career Growth
Associate → Specialist → Manager
Long-Term Outlook
Stable, technology-driven, clinically relevant
Conclusion
Identifying the best careers after biomedical engineering requires clarity on industry expectations, role realities, and long-term skill relevance. For those navigating uncertainty after graduation or early in their careers, selecting an alternative career for biomedical engineers should be a structured decision based on role clarity, industry demand, and long-term relevance rather than short-term trends.
Biomedical engineers, career growth today depends less on job titles and more on how well their skills align with evolving industry needs. Healthcare organizations increasingly seek professionals who understand systems, processes, data, and regulatory expectations. This creates meaningful opportunities beyond traditional roles for those willing to adapt and upskill with clarity. Making informed career choices, understanding role expectations early, and preparing with the right foundation can help biomedical engineers build stable and relevant careers in a changing healthcare landscape.